

Pathophysiology and management of cardiovascular disease in patients with HIV
- PMID: 26873066
- PMCID: PMC4921313
- DOI: 10.1016/S2213-8587(15)00388-5
Pathophysiology and management of cardiovascular disease in patients with HIV
Abstract
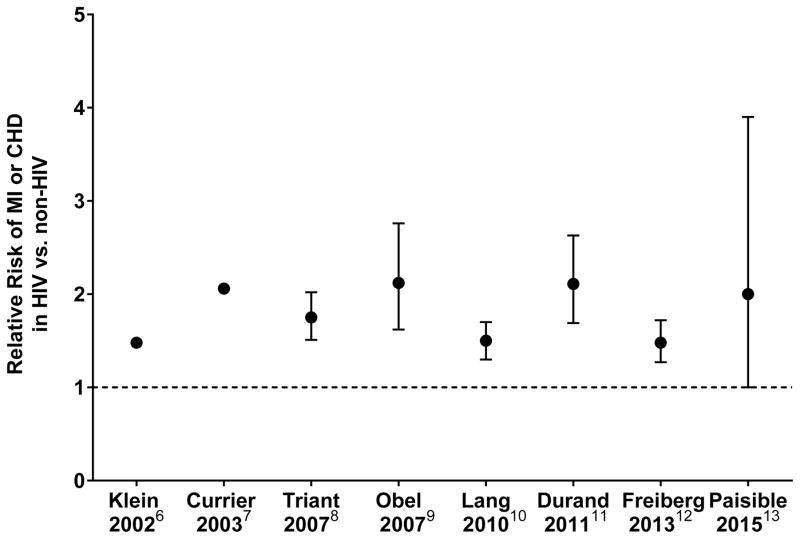
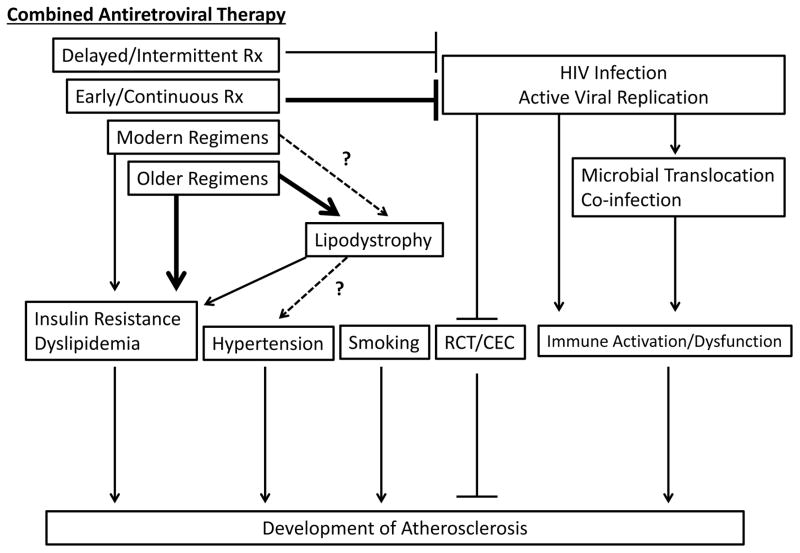
Results from several studies have suggested that people with HIV have an increased risk of cardiovascular disease, especially coronary heart disease, compared with people not infected with HIV. People living with HIV have an increased prevalence of traditional cardiovascular disease risk factors, and HIV-specific mechanisms such as immune activation. Although older, more metabolically harmful antiretroviral regimens probably contributed to the risk of cardiovascular disease, new data suggest that early and continuous use of modern regimens, which might have fewer metabolic effects, minimises the risk of myocardial infarction by maintaining viral suppression and decreasing immune activation. Even with antiretroviral therapy, however, immune activation persists in people with HIV and could contribute to accelerated atherosclerosis, especially of coronary lesions that are susceptible to rupture. Therefore, treatments that safely reduce inflammation in people with HIV could provide additional cardiovascular protection alongside treatment of both traditional and non-traditional risk factors.
Copyright © 2016 Elsevier Ltd. All rights reserved.
Conflict of interest statement
There was no role of any funding source in the creation of this review article. SKG has consulted for BMS, Merck, Navidea, Theratechnologies, Gilead, NovoNordisk, AstraZeneca, Aileron, received speaker fees from Takeda, and research funding from BMS, Gilead, Amgen, Navidea, Kowa Pharmaceuticals and Theratechnologies over the past 3 years, all unrelated to this manuscript. EN, JL, and CH have no competing interests. This work was supported in part by the National Institute of Allergies and Infectious Diseases Intramural Program. SKG is a co-investigator for the currently enrolling REPRIEVE trial.
Figures
Comment in
-
The need to focus on primary health care for chronic diseases.Lancet Diabetes Endocrinol. 2016 Sep;4(9):731-732. doi: 10.1016/S2213-8587(16)30148-6. Epub 2016 Jul 16. Lancet Diabetes Endocrinol. 2016. PMID: 27432550 No abstract available.
References
-
- WHO. HIV/AIDS: Data and Statistics [Online] 2014 [cited 2015 August 3rd]; Available from: http://www.who.int/hiv/data/en/
-
- Morlat P, Roussillon C, Henard S, Salmon D, Bonnet F, Cacoub P, et al. Causes of death among HIV-infected patients in France in 2010 (national survey): trends since 2000. AIDS. 2014;28(8):1181–91. - PubMed
-
- Hasse B, Ledergerber B, Furrer H, Battegay M, Hirschel B, Cavassini M, et al. Morbidity and aging in HIV-infected persons: the Swiss HIV cohort study. Clin Infect Dis. 2011;53(11):1130–9. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
