

Iron/folic acid supplementation during pregnancy prevents neonatal and under-five mortality in Pakistan: propensity score matched sample from two Pakistan Demographic and Health Surveys
- PMID: 26873178
- PMCID: PMC4752592
- DOI: 10.3402/gha.v9.29621
Iron/folic acid supplementation during pregnancy prevents neonatal and under-five mortality in Pakistan: propensity score matched sample from two Pakistan Demographic and Health Surveys
Abstract
Background: Several epidemiological studies from low- and middle-income countries have reported a protective effect of maternal antenatal iron/folic acid (IFA) on childhood mortality.
Objective: The current study aimed to evaluate the effect of maternal antenatal IFA supplementation on childhood mortality in Pakistan.
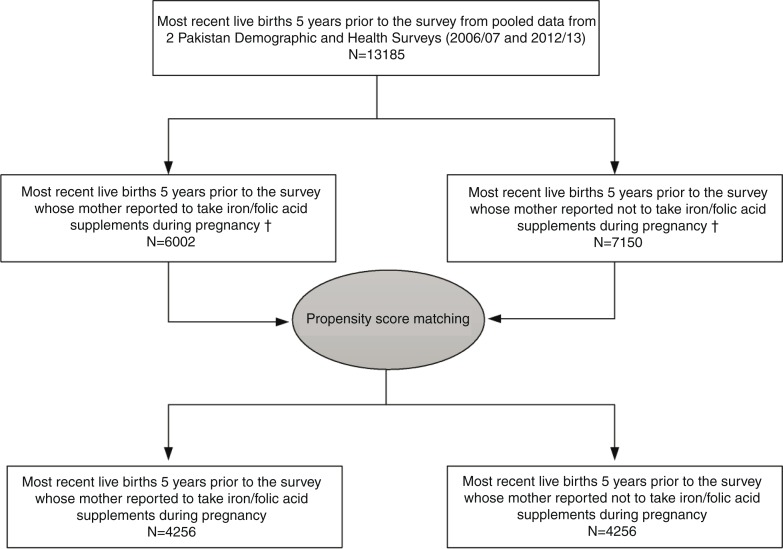
Design: A propensity score-matched sample of 8,512 infants live-born within the 5 years prior to interview was selected from the pooled data of two Pakistan Demographic and Health Surveys (2006/07 and 2012/13). The primary outcomes were childhood mortality indicators and the main exposure variable was maternal antenatal IFA supplementation. Post-matched analyses used Cox proportional hazards regression and adjusted for 16 potential confounders.
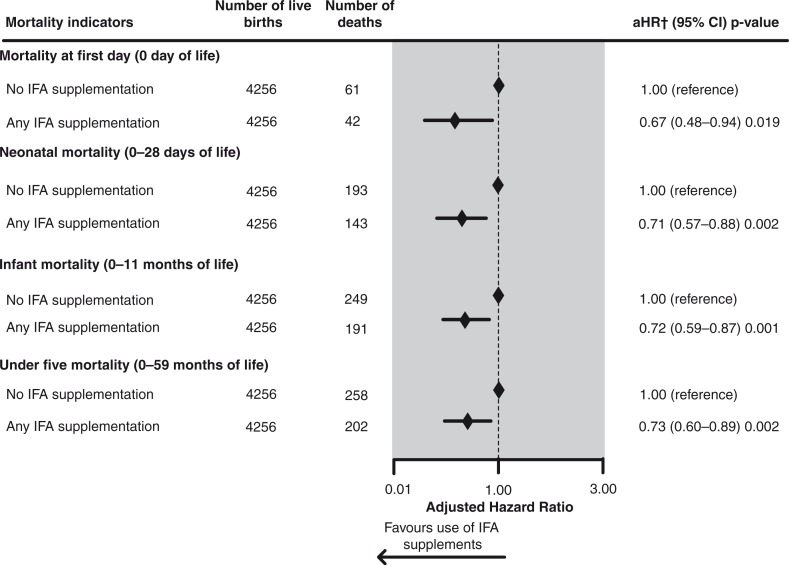
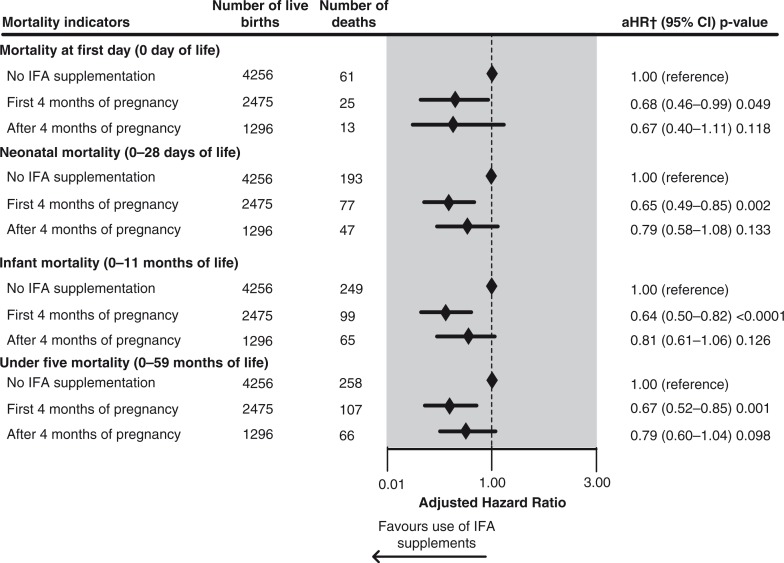
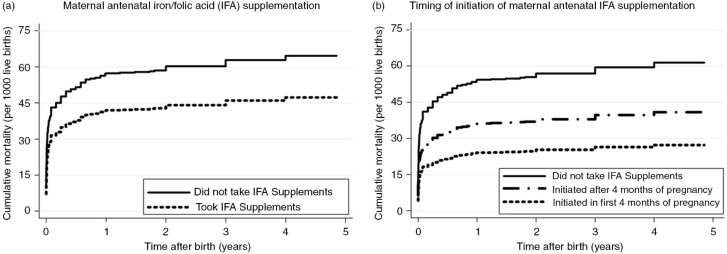
Results: Maternal antenatal IFA supplementation significantly reduced the adjusted risk of death on day 0 by 33% [adjusted hazard ratio (aHR)=0.67, 95% confidence interval (95% CI) 0.48-0.94], during the neonatal period by 29% (aHR=0.71, 95% CI 0.57-0.88), and for under-fives by 27% (aHR=0.73, 95% CI 0.60-0.89). When IFA was initiated in the first 4 months of pregnancy, the adjusted risk of neonatal and under-five deaths was significantly reduced by 35 and 33%, respectively. Twenty percent of under-five deaths were attributable to non-initiation of IFA in the first 4 months of pregnancy. With universal initiation of IFA in the first 4 months of pregnancy, 80,300 under-five deaths could be prevented annually in Pakistan.
Conclusions: Maternal antenatal IFA supplementation significantly reduced neonatal and under-five deaths in Pakistan. Earlier initiation of supplements in pregnancy was associated with a greater prevention of neonatal and under-five deaths.
Keywords: antenatal care; iron/folic acid supplements; mortality; neonatal; propensity score; under-five.
Figures
Similar articles
-
Antenatal Iron-Folic Acid Supplementation Reduces Neonatal and Under-5 Mortality in Nepal.J Nutr. 2015 Aug;145(8):1873-83. doi: 10.3945/jn.114.206565. Epub 2015 Jul 1. J Nutr. 2015. PMID: 26136588
-
Earlier initiation and use of a greater number of iron-folic acid supplements during pregnancy prevents early neonatal deaths in Nepal and Pakistan.PLoS One. 2014 Nov 14;9(11):e112446. doi: 10.1371/journal.pone.0112446. eCollection 2014. PLoS One. 2014. PMID: 25398011 Free PMC article.
-
Antenatal iron-folic acid supplementation reduces risk of low birthweight in Pakistan: secondary analysis of Demographic and Health Survey 2006-2007.Matern Child Nutr. 2016 Jan;12(1):85-98. doi: 10.1111/mcn.12156. Epub 2014 Nov 24. Matern Child Nutr. 2016. PMID: 25422133 Free PMC article.
-
Community-based distribution of iron-folic acid supplementation in low- and middle-income countries: a review of evidence and programme implications.Public Health Nutr. 2018 Feb;21(2):346-354. doi: 10.1017/S1368980017002828. Epub 2017 Oct 24. Public Health Nutr. 2018. PMID: 29061205 Free PMC article. Review.
-
Barriers and enablers for iron folic acid (IFA) supplementation in pregnant women.Matern Child Nutr. 2018 Dec;14 Suppl 5(Suppl 5):e12532. doi: 10.1111/mcn.12532. Epub 2017 Dec 22. Matern Child Nutr. 2018. PMID: 29271115 Free PMC article. Review.
Cited by
-
Intervention fidelity and its determinants of focused antenatal care package implementation, in south Wollo zone, Northeast Ethiopia.BMC Pregnancy Childbirth. 2021 Feb 19;21(1):150. doi: 10.1186/s12884-021-03637-4. BMC Pregnancy Childbirth. 2021. PMID: 33607962 Free PMC article.
-
Adherence to Iron with Folic Acid Supplementation Among Pregnant Women Attending Antenatal Care in Public Health Centers in Simada District, Northwest Ethiopia: Using Health Belief Model Perspective.Patient Prefer Adherence. 2021 Apr 21;15:843-851. doi: 10.2147/PPA.S299294. eCollection 2021. Patient Prefer Adherence. 2021. PMID: 33911855 Free PMC article.
-
Antenatal Iron-Folic Acid Supplementation Is Associated with Improved Linear Growth and Reduced Risk of Stunting or Severe Stunting in South Asian Children Less than Two Years of Age: A Pooled Analysis from Seven Countries.Nutrients. 2020 Aug 28;12(9):2632. doi: 10.3390/nu12092632. Nutrients. 2020. PMID: 32872329 Free PMC article.
-
Association between concurrence of multiple risk factors and under-5 mortality: a pooled analysis of data from Demographic and Health Survey in 61 low-and-middle-income countries.EClinicalMedicine. 2024 Apr 5;71:102583. doi: 10.1016/j.eclinm.2024.102583. eCollection 2024 May. EClinicalMedicine. 2024. PMID: 38618201 Free PMC article.
-
The Association between Iron-deficiency Anemia and Adverse Pregnancy Outcomes: A Retrospective Report from Pakistan.Cureus. 2019 Oct 7;11(10):e5854. doi: 10.7759/cureus.5854. Cureus. 2019. PMID: 31754588 Free PMC article.
References
-
- UNICEF, World Health Organization, The World Bank, United Nations, UN Inter-agency Group for Child Mortality Estimation. Levels & Trends in Child Mortality Report 2014. New York: UNICEF; 2014.
-
- National Institute of Population Studies (NIPS) [Pakistan], Macro International Inc. Pakistan Demographic and Health Survey 2012–13. Islamabad, Pakistan: NIPS, Macro International Inc; 2013.
-
- Bhutta ZA, Chopra M, Axelson H, Berman P, Boerma T, Bryce J, et al. Countdown to 2015 decade report (2000–10): taking stock of maternal, newborn, and child survival. Lancet. 2010;375:2032–44. - PubMed
-
- Khan A, Kinney MV, Hazir T, Hafeez A, Wall SN, Ali N, et al. Newborn survival in Pakistan: a decade of change and future implications. Health Policy Plan. 2012;27:iii72–iii87. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical