

Percutaneous Patent Ductus Arteriosus (PDA) Closure in Very Preterm Infants: Feasibility and Complications
- PMID: 26873689
- PMCID: PMC4802484
- DOI: 10.1161/JAHA.115.002923
Percutaneous Patent Ductus Arteriosus (PDA) Closure in Very Preterm Infants: Feasibility and Complications
Abstract
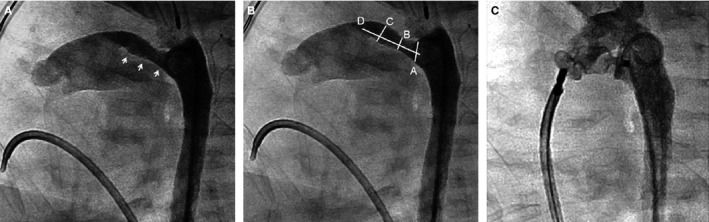
Background: Percutaneous closure of patent ductus arteriosus (PDA) in term neonates is established, but data regarding outcomes in infants born very preterm (<32 weeks of gestation) are minimal, and no published criteria exist establishing a minimal weight of 4 kg as a suitable cutoff. We sought to analyze outcomes of percutaneous PDA occlusion in infants born very preterm and referred for PDA closure at weights <4 kg.
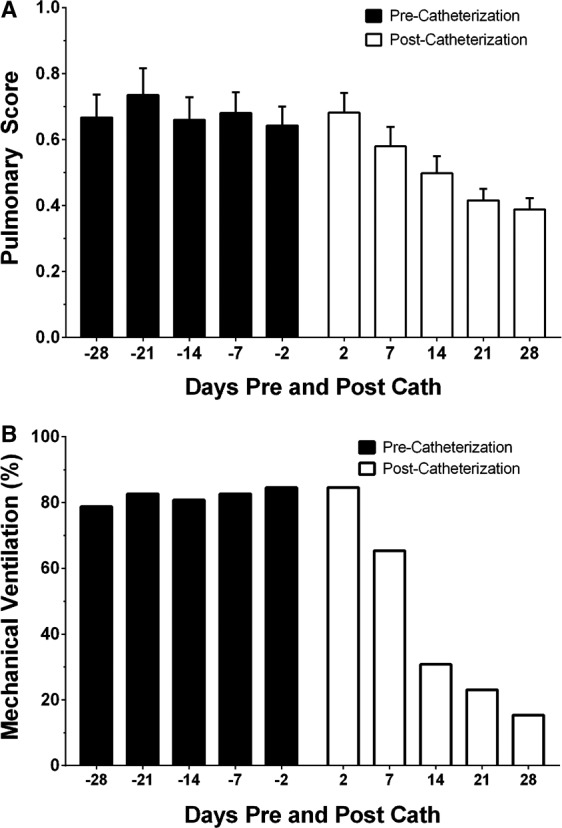
Methods and results: Retrospective analysis (January 2005-January 2014) was done at a single pediatric center. Procedural successes and adverse events were recorded. Markers of respiratory status (need for mechanical ventilation) were determined, with comparisons made before and after catheterization. A total of 52 very preterm infants with a median procedural weight of 2.9 kg (range 1.2-3.9 kg) underwent attempted PDA closure. Twenty-five percent (13/52) of infants were <2.5 kg. Successful device placement was achieved in 46/52 (88%) of infants. An adverse event occurred in 33% of cases, with an acute arterial injury the most common complication. We observed no association between weight at time of procedure and the risk of an adverse event. No deaths were attributable to the PDA closure. Compared to precatheterization trends, percutaneous PDA closure resulted in improved respiratory status, including less exposure to mechanical ventilation (mixed effects logistic model, P<0.01).
Conclusions: Among infants born very preterm, percutaneous PDA closure at weights <4 kg is generally safe and may improve respiratory health, but risk of arterial injury is noteworthy. Randomized clinical trials are needed to assess clinically relevant differences in outcomes following percutaneous PDA closure versus alternative (surgical ligation) management strategies.
Keywords: arterial thrombosis; catheterization; complications; ductus arteriosus, patent; neonatal; pediatrics.
© 2016 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley Blackwell.
Figures
References
-
- Dollberg S, Lusky A, Reichman B. Patent ductus arteriosus, indomethacin and necrotizing enterocolitis in very low birth weight infants: a population‐based study. J Pediatr Gastroenterol Nutr. 2005;40:184–188. - PubMed
-
- Sellmer A, Bjerre JV, Schmidt MR, McNamara PJ, Hjortdal VE, Host B, Bech BH, Henriksen TB. Morbidity and mortality in preterm neonates with patent ductus arteriosus on day 3. Arch Dis Child Fetal Neonatal Ed. 2013;98:F505–F510. - PubMed
-
- Hoffman JI, Kaplan S. The incidence of congenital heart disease. J Am Coll Cardiol. 2002;39:1890–1900. - PubMed
-
- Noori S, McCoy M, Friedlich P, Bright B, Gottipati V, Seri I, Sekar K. Failure of ductus arteriosus closure is associated with increased mortality in preterm infants. Pediatrics. 2009;123:e138–e144. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
