

Adherence to Antihypertensive Medication in Treatment-Resistant Hypertension Undergoing Renal Denervation
- PMID: 26873693
- PMCID: PMC4802436
- DOI: 10.1161/JAHA.115.002343
Adherence to Antihypertensive Medication in Treatment-Resistant Hypertension Undergoing Renal Denervation
Abstract
Background: Adherence to medication has been repeatedly proposed to represent a major cause of treatment-resistant hypertension (TRH); however, treatment decisions such as treating TRH with renal denervation depend on accurate judgment of adherence. We carefully analyzed adherence rates to medication before and after renal denervation and its effect on blood pressure (BP) control.
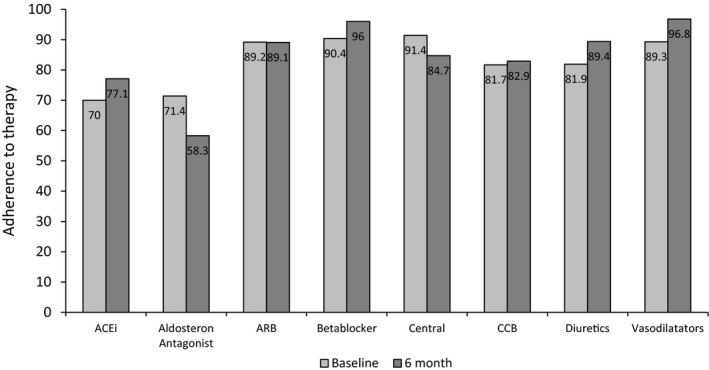
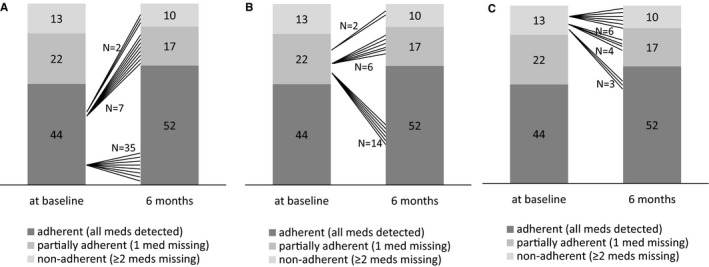
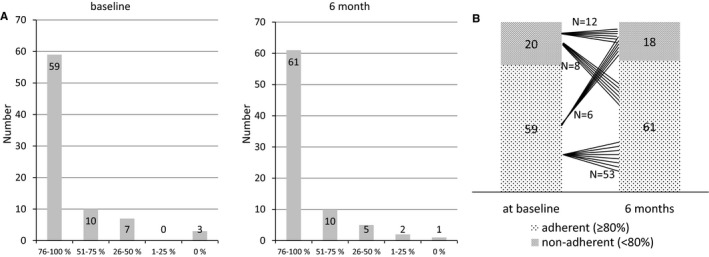
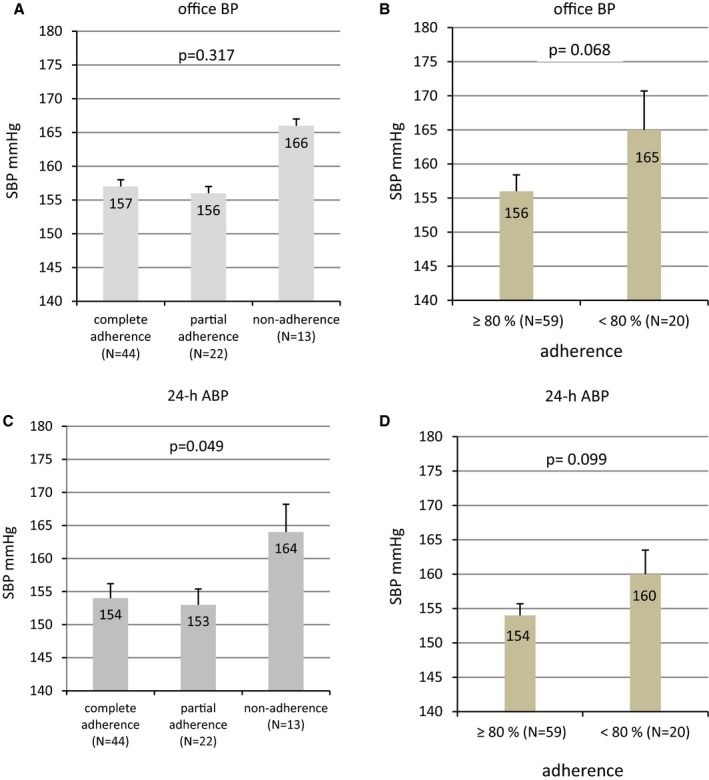
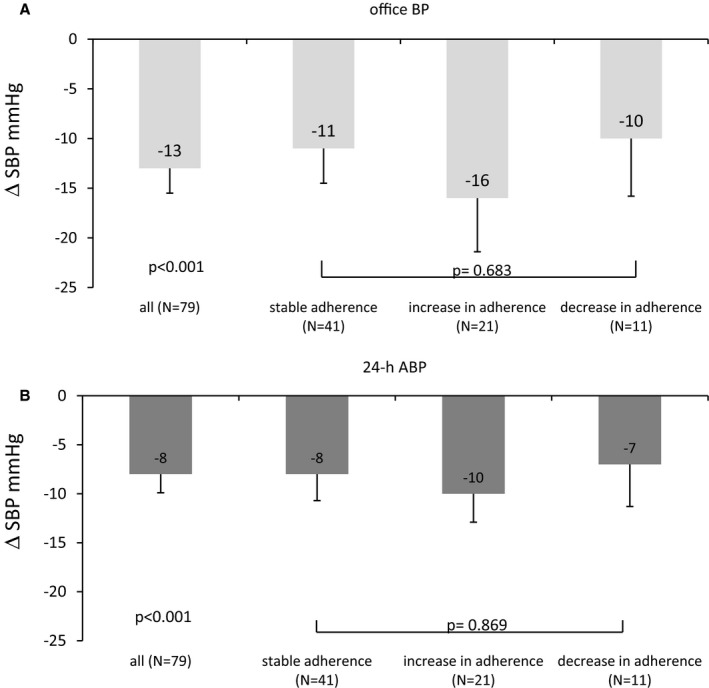
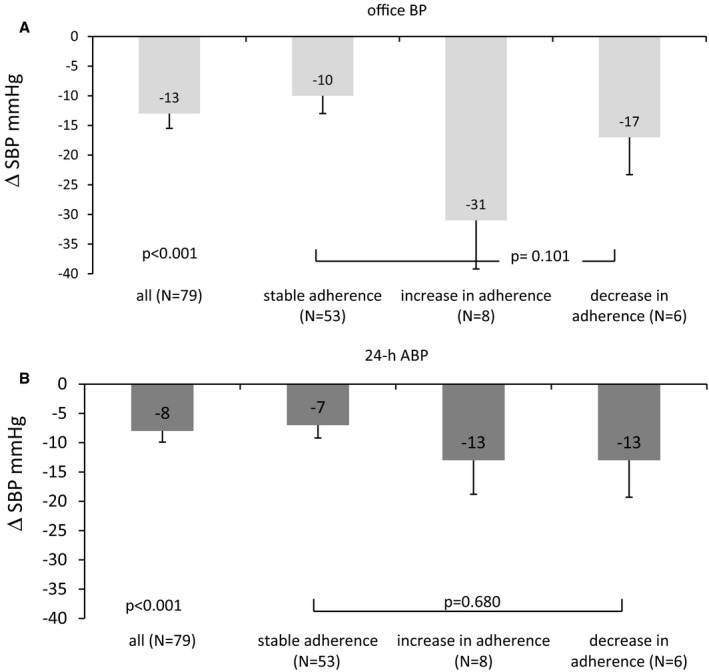
Methods and results: Eighty patients with TRH were included in 2 prospective observational studies that assessed the difference of potential antihypertensive and nephroprotective effects of renal denervation. To compare prescribed with actual medication intake (representing a measure of adherence), we analyzed urine samples collected at baseline and at 6 months after renal denervation for antihypertensive compounds or metabolites (by liquid chromatography-mass spectrometry). In addition to office BP, 24-hour ambulatory BP and central hemodynamics (central systolic pressure, central pulse pressure) were assessed. Informed consent for analyses of urine metabolites was obtained from 79 of 80 patients. Actual intake of all antihypertensive drugs was detected at baseline and at 6 months after renal denervation in 44 (56%) and 52 (66%) patients, respectively; 1 drug was missing in 22 (28%) and 17 (22%) patients, respectively, and ≥2 drugs were missing in 13 (16%) and 10 (13%) patients, respectively. At baseline, 24-hour ambulatory BP (P=0.049) and central systolic BP (P=0.012) were higher in nonadherent patients. Adherence did not significantly change overall (McNemar-Bowker test, P=0.362). An increase in adherence was observed in 21 patients, and a decrease was observed in 11 patients. The decrease in 24-hour ambulatory BP was not different in those with stable adherence 6 months after renal denervation (n=41, -7±13 mm Hg) compared with those with increased adherence (n=21, -10±13 mm Hg) and decreased adherence (n=11, -7±14 mm Hg) (P>0.20). Our study is limited by the relatively small sample size and potentially by the specific health environment of our university center (Northern Bavaria, Germany).
Conclusions: Nonadherence to medication among patients with TRH was relatively low: ≈1 of 6 patients with TRH did not take ≥2 of the prescribed drugs. Adherence pattern did not change significantly after renal denervation and had no impact on the overall observed BP changes, supporting the concept that renal denervation is an effective treatment in patients with TRH.
Clinical trial registration: URL: https://www.clinicaltrials.gov. Unique identifiers: NCT00888433, NCT01442883 and NCT01687725.
Keywords: adherence; antihypertensive medication; renal denervation; resistant hypertension; treatment.
© 2016 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley Blackwell.
Figures
Similar articles
-
Adherence to Antihypertensive Treatment and the Blood Pressure-Lowering Effects of Renal Denervation in the Renal Denervation for Hypertension (DENERHTN) Trial.Circulation. 2016 Sep 20;134(12):847-57. doi: 10.1161/CIRCULATIONAHA.116.022922. Epub 2016 Aug 30. Circulation. 2016. PMID: 27576780 Clinical Trial.
-
Renal sympathetic denervation in patients with treatment-resistant hypertension after witnessed intake of medication before qualifying ambulatory blood pressure.Hypertension. 2013 Sep;62(3):526-32. doi: 10.1161/HYPERTENSIONAHA.113.01452. Epub 2013 Jul 8. Hypertension. 2013. PMID: 23836798
-
Impact of Medication Adherence on the Effect of Renal Denervation: The SYMPATHY Trial.Hypertension. 2017 Apr;69(4):678-684. doi: 10.1161/HYPERTENSIONAHA.116.08818. Hypertension. 2017. PMID: 28264922 Clinical Trial.
-
Renal sympathetic denervation after Symplicity HTN-3 and therapeutic drug monitoring in patients with resistant hypertension to improve patients' adherence.Eur Heart J Cardiovasc Pharmacother. 2015 Jan;1(1):48-56. doi: 10.1093/ehjcvp/pvu009. Eur Heart J Cardiovasc Pharmacother. 2015. PMID: 27533966 Review.
-
Impact of renal denervation on quality of life (How does renal denervation contribute to improving hypertension treatment affected by poor medication adherence?).Hypertens Res. 2024 Oct;47(10):2652-2658. doi: 10.1038/s41440-024-01679-7. Epub 2024 Apr 11. Hypertens Res. 2024. PMID: 38605140 Review.
Cited by
-
Clinical trials in neuromodulatory treatment of drug-resistant hypertension and the need for spinal cord stimulation trials: a PRISMA systematic review.Bioelectron Med. 2024 Dec 2;10(1):28. doi: 10.1186/s42234-024-00160-7. Bioelectron Med. 2024. PMID: 39617923 Free PMC article. Review.
-
The psychosocial barriers to medication adherence of patients with type 2 diabetes: a qualitative study.Biopsychosoc Med. 2021 Jan 18;15(1):1. doi: 10.1186/s13030-020-00202-x. Biopsychosoc Med. 2021. PMID: 33461565 Free PMC article.
-
Facing the Challenge of Lowering Blood Pressure and Cholesterol in the Same Patient: Report of a Symposium at the European Society of Hypertension.Cardiol Ther. 2020 Jun;9(1):19-34. doi: 10.1007/s40119-019-00159-1. Epub 2020 Jan 13. Cardiol Ther. 2020. PMID: 31933276 Free PMC article. Review.
-
A study on usefulness of modified medication adherence scale in assessing adherence among hypertensive patients.Perspect Clin Res. 2019 Oct-Dec;10(4):163-167. doi: 10.4103/picr.PICR_44_18. Perspect Clin Res. 2019. PMID: 31649865 Free PMC article.
-
GLP-1-based therapies for the treatment of resistant hypertension in individuals with overweight or obesity: a review.EClinicalMedicine. 2024 Aug 15;75:102789. doi: 10.1016/j.eclinm.2024.102789. eCollection 2024 Sep. EClinicalMedicine. 2024. PMID: 39246720 Free PMC article. Review.
References
-
- Osterberg L, Blaschke T. Adherence to medication. N Engl J Med. 2005;353:487–497. - PubMed
-
- Hill MN, Miller NH, Degeest S; American Society of Hypertension Writing G , Materson BJ, Black HR, Izzo JL Jr, Oparil S, Weber MA. Adherence and persistence with taking medication to control high blood pressure. J Am Soc Hypertens. 2011;5:56–63. - PubMed
-
- Burnier M. Managing ‘resistance’: is adherence a target for treatment? Curr Opin Nephrol Hypertens. 2014;23:439–443. - PubMed
-
- Mancia G, Zambon A, Soranna D, Merlino L, Corrao G. Factors involved in the discontinuation of antihypertensive drug therapy: an analysis from real life data. J Hypertens. 2014;32:1708–1715; discussion 1716. - PubMed
-
- Corrao G, Parodi A, Nicotra F, Zambon A, Merlino L, Cesana G, Mancia G. Better compliance to antihypertensive medications reduces cardiovascular risk. J Hypertens. 2011;29:610–618. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
