Clinical Practices and Outcomes on Chemotherapy-Induced Nausea and Vomiting Management in South Korea: Comparison with Asia-Pacific Data of the Pan Australasian Chemotherapy Induced Emesis Burden of Illness Study
- PMID: 26875197
- PMCID: PMC5080826
- DOI: 10.4143/crt.2015.309
Clinical Practices and Outcomes on Chemotherapy-Induced Nausea and Vomiting Management in South Korea: Comparison with Asia-Pacific Data of the Pan Australasian Chemotherapy Induced Emesis Burden of Illness Study
Abstract
Purpose: This study reported patient outcomes of chemotherapy-induced nausea and vomiting (CINV) prophylaxis for highly emetogenic chemotherapy (HEC) and moderately emetogenic chemotherapy (MEC) regimens and evaluated its adherence to acute-phase CINV prophylaxis in the Korean population subset of the Pan Australasian Chemotherapy Induced Emesis burden of illness (PrACTICE) study.
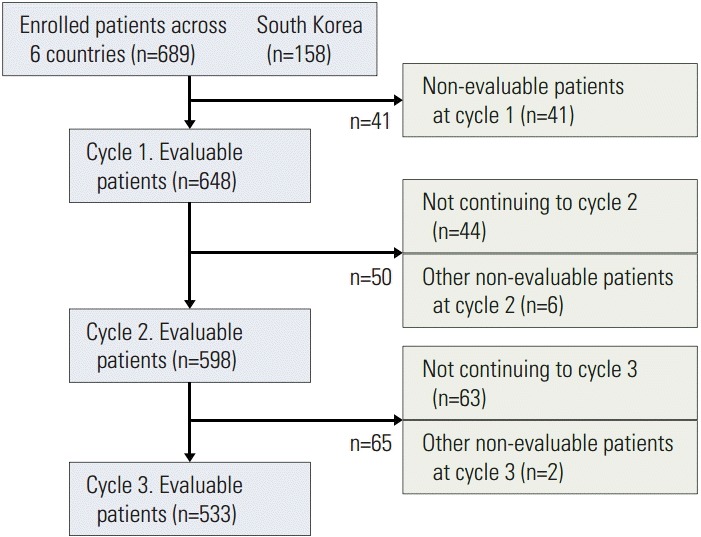
Materials and methods: This subgroup analysis evaluated 158 Korean patients receiving HEC or MEC and compared the data (wherever possible) with that of 648 patients from the Asia-Pacific (AP) region. Study endpoints included evaluation of primary CINV prophylaxis and adherence to acute-phase CINV prophylaxis in cycle 1 (American Society of Clinical Oncology [ASCO] Quality Oncology Practice Initiative [QOPI]).
Results: In South Korea and the AP, a 5-hydroxytryptamine-3 receptor antagonist (5HT3-RA) prophylaxis for the acute phase was administered to 79/80 patients (98.8%) for HEC and 70/71 patients (98.6%) for MEC regimens (QOPI-1). Triple regimen (corticosteroid-5HT3-RA-neurokinin 1-RA) was initiated in 46/80 patients (57.5%) for prophylaxis of acute CINV in cycle 1 of HEC (QOPI-3). Double regimen (corticosteroid-5HT3-RA, with or within NK1-RA) was initiated in 61/71 patients (83.1%) for control of acute CINV in cycle 1 of MEC a(QOPI-2).
Conclusion: Active management of CINV is necessary in cycle 1 of HEC in South Korea, despite higher rates than the AP region. Adherence to the international guidelines for CINV prophylaxis requires attention in the acute phase in cycle 1 of the HEC regimen.
Keywords: Antiemetics; Drug therapy; Nausea; Vomiting.
Conflict of interest statement
This study was funded by Merck & Co., Inc. Medical writing services were provided by Dr. Annirudha Chillar of Cactus Communications and funded by Merck & Co., Inc. The authors retained full control of the manuscript content.
Figures
References
-
- Jordan K, Gralla R, Jahn F, Molassiotis A. International antiemetic guidelines on chemotherapy induced nausea and vomiting (CINV): content and implementation in daily routine practice. Eur J Pharmacol. 2014;722:197–202. - PubMed
-
- Bloechl-Daum B, Deuson RR, Mavros P, Hansen M, Herrstedt J. Delayed nausea and vomiting continue to reduce patients' quality of life after highly and moderately emetogenic chemotherapy despite antiemetic treatment. J Clin Oncol. 2006;24:4472–8. - PubMed
-
- Hassan BA, Yusoff ZB. Genetic polymorphisms in the three malaysian races effect granisetron clinical antiemetic actions in breast cancer patients receiving chemotherapy. Asian Pac J Cancer Prev. 2011;12:185–91. - PubMed
-
- Molassiotis A, Aapro M, Dicato M, Gascon P, Novoa SA, Isambert N, et al. Evaluation of risk factors predicting chemotherapy-related nausea and vomiting: results from a European prospective observational study. J Pain Symptom Manage. 2014;47:839–48. e4. - PubMed
-
- Pirri C, Katris P, Trotter J, Bayliss E, Bennett R, Drummond P. Risk factors at pretreatment predicting treatment-induced nausea and vomiting in Australian cancer patients: a prospective, longitudinal, observational study. Support Care Cancer. 2011;19:1549–63. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical