

Niacin Alternatives for Dyslipidemia: Fool's Gold or Gold Mine? Part I: Alternative Niacin Regimens
- PMID: 26876225
- PMCID: PMC4753247
- DOI: 10.1007/s11883-016-0563-8
Niacin Alternatives for Dyslipidemia: Fool's Gold or Gold Mine? Part I: Alternative Niacin Regimens
Abstract
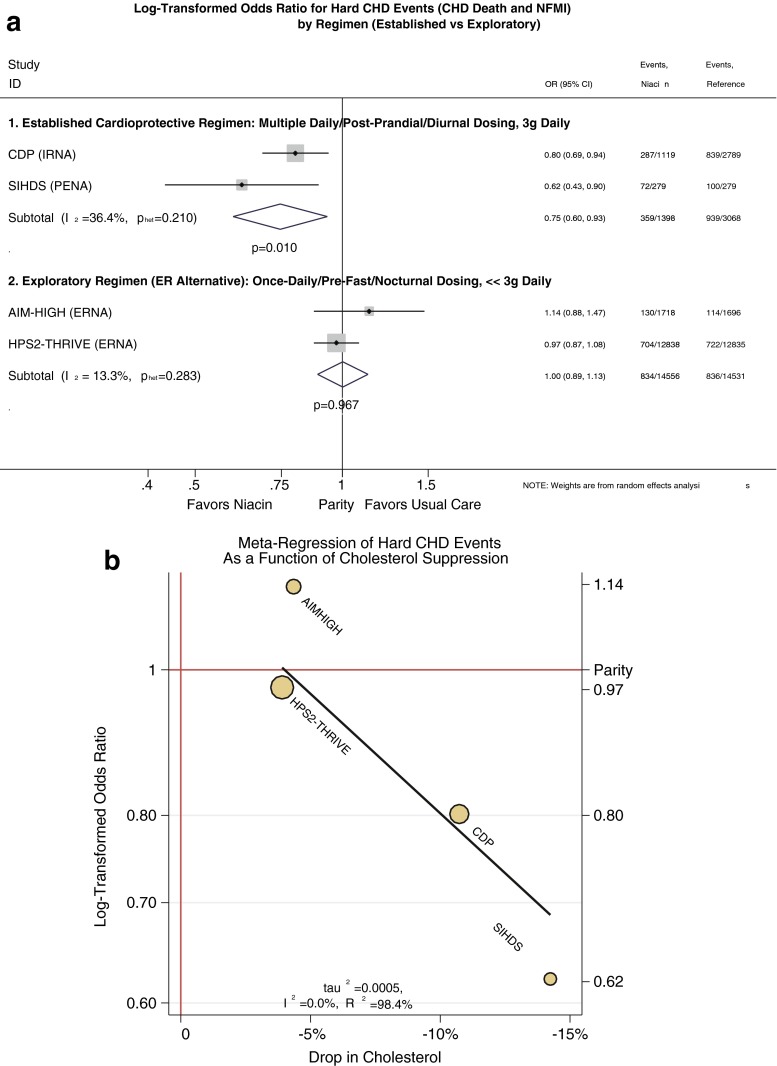
Niacin was the first drug demonstrating lowered cholesterol prevents coronary heart disease (CHD) events, with two clinical CHD outcome studies establishing a cardioprotective niacin regimen: 1 g thrice daily with meals. Though cardioprotective, skin toxicity limits niacin's use, fostering several variations to improve tolerability. One of these, an extended-release (ER) alternative, proved immensely successful commercially, dominating clinical practice despite departing from the established regimen in several critical ways. Hence, improved tolerability may have come at the cost of diminished efficacy, posing a conundrum: Does it still help the population at risk for CHD to broaden a drug's acceptance by "watering it down"? This question is crucial at this stage now that the ER alternative failed to recapitulate the benefits of the established cardioprotective niacin regimen in two trials of the alternative approach: AIM-HIGH and HPS2-THRIVE. Part I of this review discusses how vastly the ER alternative departs from the established cardioprotective regimen, why that is important physiologically, and how it may explain the findings of AIM-HIGH and HPS2-THRIVE. Given important gaps left by statin therapy, the established cardioprotective niacin regimen remains an important evidence-based therapy for the statin intolerant or statin averse.
Keywords: Hyperlipidemia; Lipids; Niacin; Niacin conjugates; Niacin prodrugs; Nicotinic acid.
Figures


References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
