

Endoscopic Repair of CSF Rhinorrhea: An Institutional Experience
- PMID: 26878002
- PMCID: PMC4735615
Endoscopic Repair of CSF Rhinorrhea: An Institutional Experience
Abstract
Introduction: Endoscopic repair is considered the treatment of choice in cerebrospinal fluid (CSF) rhinorrhea. The aim of our study was to analyze the etiopathogenesis of CSF rhinorrhea, the outcome of treatment and the causes of failure in a developing-country setting.
Materials and methods: A retrospective review of patients treated with endoscopic repair for CSF rhinorrhea at a tertiary care hospital in southern India from January 2002 to December 2009 identified 36 patients, the majority of them being women. The defects were closed in three layers using fat, fascia lata and nasal mucosa along with a fibrin sealant in the majority of the patients. Per-operatively, a subarachnoid drain was placed in all patients. Patients were followed up for 1 year.
Results: Spontaneous onset of CSF rhinorrhea was noted in 61% of patients. The most common site of leak was found to be the left cribriform plate area. Hence the most common cause of CSF rhinorrhea in our study was spontaneous and the second most common was post-traumatic. Our success rate on the first attempt at endoscopic repair was 100%, with a recurrence rate of 6%. A large defect, failure of localization of the defect, or other co-morbid conditions such as chronic cough may be the most likely causes of recurrence of leak.
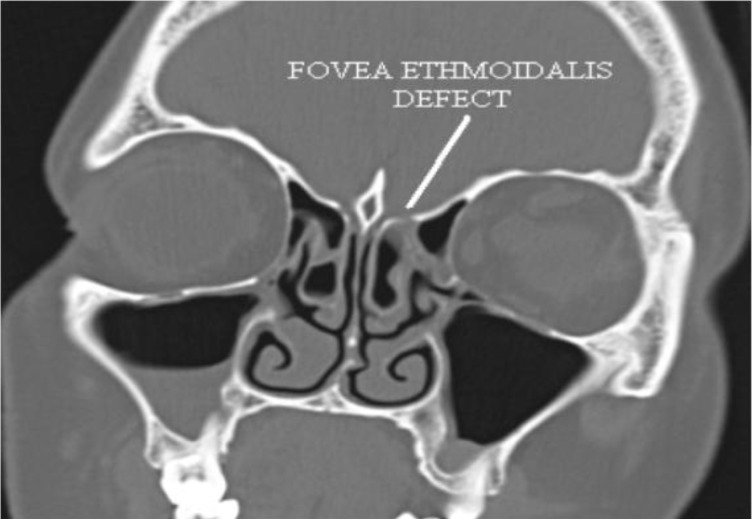
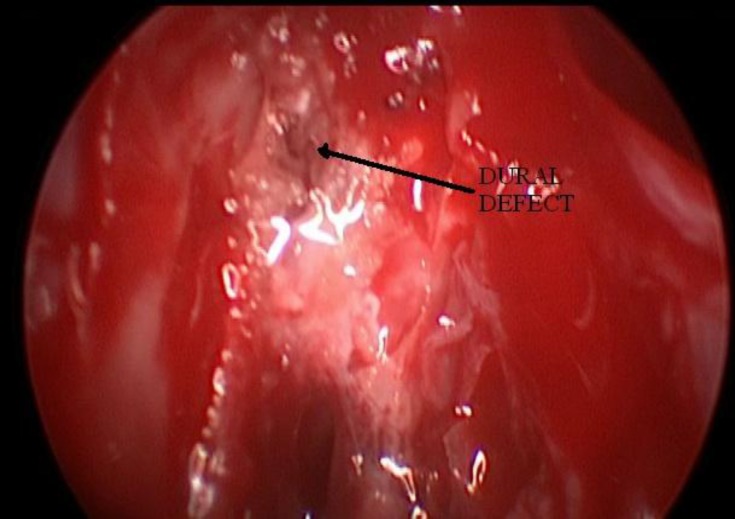
Conclusion: Accurate localization of the site of lesion using a high-resolution computed tomography (CT) scan with magnetic resonance imaging (MRI) and confirmation of the site of leak by intraoperative Valsalva maneuver along with multilayered closure of the dural defect and post-operative lumbar drain appear to be essential for the successful endoscopic repair of CSF rhinorrhea.
Keywords: CSF rhinorrhea; Cribriform plate; Subarachnoid Space; Transnasal Endoscopic Surgery; Valsalva Maneuver.
Figures
Similar articles
-
Trans-Nasal Endoscopic Repair of CSF Rhinorrhea: An Institutional Experience.Indian J Otolaryngol Head Neck Surg. 2024 Feb;76(1):748-752. doi: 10.1007/s12070-023-04267-2. Epub 2023 Oct 13. Indian J Otolaryngol Head Neck Surg. 2024. PMID: 38440577 Free PMC article.
-
Factors That Predict Recurrence Following Endoscopic Repair of Cerebrospinal Fluid Rhinorrhea.World Neurosurg. 2024 May;185:e532-e541. doi: 10.1016/j.wneu.2024.02.069. Epub 2024 Feb 17. World Neurosurg. 2024. PMID: 38373688
-
Endoscopic management of CSF rhinorrhea.Neurol India. 2014 Sep-Oct;62(5):532-9. doi: 10.4103/0028-3886.144453. Neurol India. 2014. PMID: 25387624
-
Traumatic, iatrogenic, and spontaneous cerebrospinal fluid (CSF) leak: endoscopic repair.B-ENT. 2011;7 Suppl 17:47-60. B-ENT. 2011. PMID: 22338375 Review.
-
Endoscopic repair of cerebrospinal fluid rhinorrhoea.Eur Ann Otorhinolaryngol Head Neck Dis. 2016 Jun;133(3):187-90. doi: 10.1016/j.anorl.2015.05.010. Epub 2016 Jan 6. Eur Ann Otorhinolaryngol Head Neck Dis. 2016. PMID: 26776882 Review.
Cited by
-
Spontaneous Cerebrospinal Fluid Rhinorrhea in End Stage Renal Disease.Indian J Nephrol. 2021 May-Jun;31(3):296-298. doi: 10.4103/ijn.IJN_372_19. Epub 2021 Mar 27. Indian J Nephrol. 2021. PMID: 34376948 Free PMC article.
-
Risk factors for postoperative cerebrospinal fluid leakage after transsphenoidal surgery for pituitary adenoma: a meta-analysis and systematic review.BMC Neurol. 2021 Oct 27;21(1):417. doi: 10.1186/s12883-021-02440-0. BMC Neurol. 2021. PMID: 34706659 Free PMC article.
-
Endonasal endoscopic repair of cerebrospinal fluid leaks versus craniotomy: comparison of the outcomes.Hippokratia. 2016 Oct-Dec;20(4):299-302. Hippokratia. 2016. PMID: 29416303 Free PMC article.
-
Endoscopic Repair of CSF Fistulae: A Ten Year Experience.J Clin Diagn Res. 2016 Aug;10(8):MC01-4. doi: 10.7860/JCDR/2016/18903.8390. Epub 2016 Aug 1. J Clin Diagn Res. 2016. PMID: 27656471 Free PMC article.
-
Management of recurrent cerebrospinal fluid leak, current practices and open challenges. A systematic literature review.Acta Otorhinolaryngol Ital. 2023 Apr;43(Suppl 1):S14-S27. doi: 10.14639/0392-100X-suppl.1-43-2023-02. Acta Otorhinolaryngol Ital. 2023. PMID: 37698096 Free PMC article. Review.
References
-
- Park J-I, Strelzow W, Friedman WH. Current management of cerebrospinal fluid rhinorrhoea. Laryngoscope. 1983;93:1294–300. - PubMed
-
- Banks CA, Palmer JN, Chiu AG, O'Malley BW Jr, Woodworth BA, Kennedy DW. Endoscopic closure of CSF rhinorrhea: 193 cases over 21 years. Otolaryngol Head Neck Surg. 2009;140(6):826–33. - PubMed
-
- Eljamel MS, Foy PM. Non-traumatic CSF fistulae: Clinical history and management. Br J Neurosurg. 1991;5:275–9. - PubMed
-
- Lund VJ, Savy L, Lloyd G, Howard D. Optimum imaging and diagnosis of cerebrospinal fluid rhinorrhea. J Laryngol Otol. 2000;114:988–92. - PubMed
LinkOut - more resources
Full Text Sources