

International multicenter comparative trial of transluminal EUS-guided biliary drainage via hepatogastrostomy vs. choledochoduodenostomy approaches
- PMID: 26878045
- PMCID: PMC4751013
- DOI: 10.1055/s-0041-109083
International multicenter comparative trial of transluminal EUS-guided biliary drainage via hepatogastrostomy vs. choledochoduodenostomy approaches
Abstract
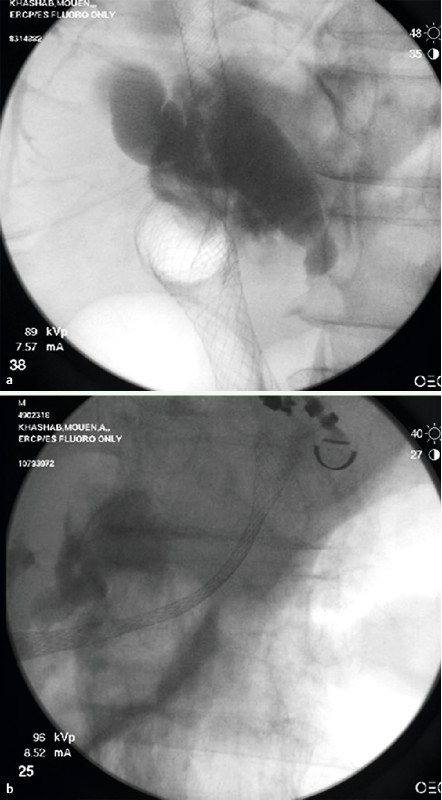
Background and study aims: Endoscopic ultrasound-guided biliary drainage (EUS-BD) can be performed entirely transgastrically (hepatogastrostomy/EUS-HG) or transduodenally (choledochoduodenostomy/EUS-CDS). It is unknown how both techniques compare. The aims of this study were to compare efficacy and safety of both techniques and identify predictors of adverse events.
Patients and methods: Consecutive jaundiced patients with distal malignant biliary obstruction who underwent EUS-BD at multiple international centers were included. Technical/clinical success, adverse events, stent complications, and survival were assessed.
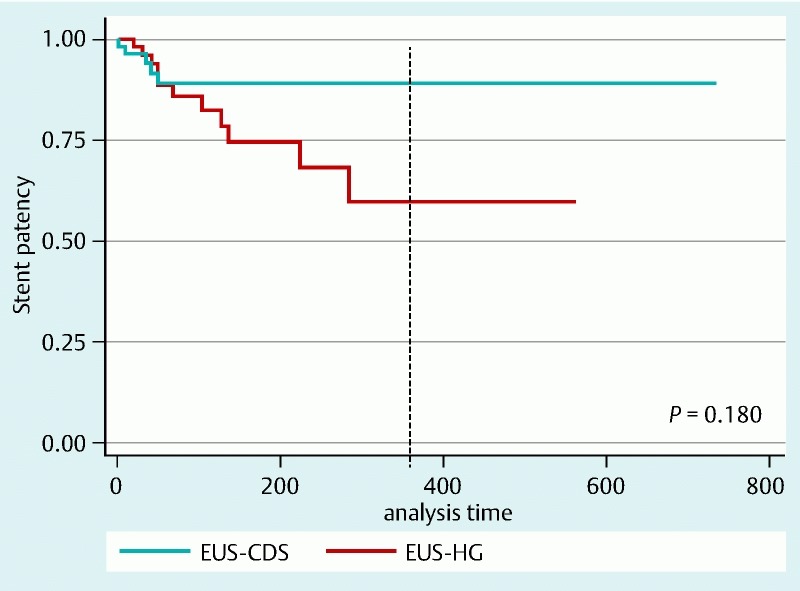
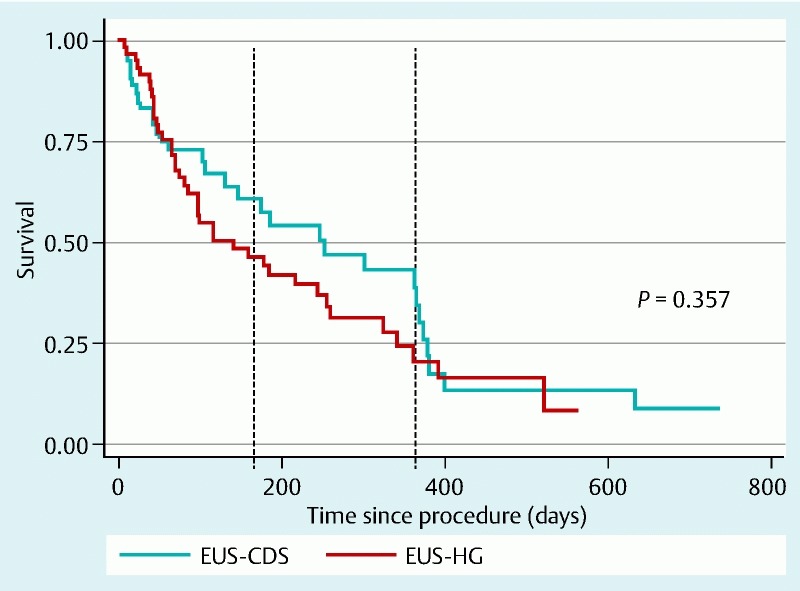
Results: A total of 121 patients underwent EUS-BD (CDS 60, HG 61). Technical success was achieved in 112 (92.56 %) patients (EUS-CDS 93.3 %, EUS-HG 91.8 %, P = 0.75). Clinical success was attained in 85.5 % of patients who underwent EUS-CDS group as compared to 82.1 % of patients who underwent EUS-HG (P = 0.64). Adverse events occurred more commonly in the EUS-HG group (19.67 % vs. 13.3 %, P = 0.37). Both plastic stenting (OR 4.95, 95 %CI 1.41 - 17.38, P = 0.01) and use of non-coaxial electrocautery (OR 3.95, 95 %CI 1.16 - 13.40, P = 0.03) were independently associated with adverse events. Length of hospital stay was significantly shorter in the CDS group (5.6 days vs. 12.7 days, P < 0.001). Mean follow-up duration was 151 ± 159 days. The 1-year stent patency probability was greater in the EUS-CDS group [0.98 (95 %CI 0.76 - 0.96) vs 0.60 (95 %CI 0.35 - 0.78)] but overall patency was not significantly different. There was no difference in median survival times between the groups (P = 0.36) CONCLUSIONS: Both EUS-CDS and EUS-HG are effective and safe techniques for the treatment of distal biliary obstruction after failed ERCP. However, CDS is associated with shorter hospital stay, improved stent patency, and fewer procedure- and stent-related complications. Metallic stents should be placed whenever feasible and non-coaxial electrocautery should be avoided when possible as plastic stenting and non-coaxial electrocautery were independently associated with occurrence of adverse events.
Conflict of interest statement
Figures
Similar articles
-
Lumen apposing metal stents versus tubular self-expandable metal stents for endoscopic ultrasound-guided choledochoduodenostomy in malignant biliary obstruction.Surg Endosc. 2021 Dec;35(12):6754-6762. doi: 10.1007/s00464-020-08179-y. Epub 2020 Nov 30. Surg Endosc. 2021. PMID: 33258038
-
EUS-guided biliary drainage with transluminal stenting after failed ERCP: predictors of adverse events and long-term results.Gastrointest Endosc. 2011 Dec;74(6):1276-84. doi: 10.1016/j.gie.2011.07.054. Epub 2011 Oct 1. Gastrointest Endosc. 2011. PMID: 21963067
-
Comparison of long-term outcomes of endoscopic ultrasound-guided hepaticogastrostomy and choledochoduodenostomy for distal malignant biliary obstruction: a multicenter retrospective study.Therap Adv Gastroenterol. 2024 Mar 19;17:17562848241239551. doi: 10.1177/17562848241239551. eCollection 2024. Therap Adv Gastroenterol. 2024. PMID: 38510458 Free PMC article.
-
EUS-guided Choledochoduodenostomy Versus Hepaticogastrostomy: A Systematic Review and Meta-analysis.J Clin Gastroenterol. 2018 Feb;52(2):123-130. doi: 10.1097/MCG.0000000000000948. J Clin Gastroenterol. 2018. PMID: 29095426
-
EUS-guided biliary drainage versus ERCP for first-line palliation of malignant distal biliary obstruction: A systematic review and meta-analysis.Sci Rep. 2019 Nov 12;9(1):16551. doi: 10.1038/s41598-019-52993-x. Sci Rep. 2019. PMID: 31719562 Free PMC article.
Cited by
-
Therapeutic endoscopic ultrasound.Transl Gastroenterol Hepatol. 2022 Apr 25;7:20. doi: 10.21037/tgh-2020-12. eCollection 2022. Transl Gastroenterol Hepatol. 2022. PMID: 35548470 Free PMC article. Review.
-
EUS-Guided Hepatico-Gastrostomy: To Dilate or Not to Dilate?Dig Dis Sci. 2022 Dec;67(12):5366-5367. doi: 10.1007/s10620-022-07560-2. Epub 2022 Jun 10. Dig Dis Sci. 2022. PMID: 35689109 No abstract available.
-
Outcomes of EUS-guided choledochoduodenostomy as primary drainage for distal biliary obstruction with covered self-expandable metallic stents.Endosc Int Open. 2020 Jul;8(7):E861-E868. doi: 10.1055/a-1161-8488. Epub 2020 Jun 16. Endosc Int Open. 2020. PMID: 32617390 Free PMC article.
-
A novel tapered plastic stent with an ultrafine delivery system for one-step endoscopic ultrasound-guided hepaticogastrostomy.Endoscopy. 2023 Dec;55(S 01):E354-E355. doi: 10.1055/a-1992-5535. Epub 2023 Jan 16. Endoscopy. 2023. PMID: 36646123 Free PMC article. No abstract available.
-
Endoscopic ultrasound-guided biliary drainage for distal malignant obstruction: a systematic review and meta-analysis of randomized trials.Endosc Int Open. 2019 Nov;7(11):E1563-E1573. doi: 10.1055/a-0998-8129. Epub 2019 Nov 11. Endosc Int Open. 2019. PMID: 31723579 Free PMC article.
References
-
- Khashab M A, Varadarajulu S. Endoscopic ultrasonography as a therapeutic modality. Curr Opin Gastroenterol. 2012;28:467–476. - PubMed
-
- Kahaleh M, Hernandez A J, Tokar J et al.Interventional EUS-guided cholangiography: evaluation of a technique in evolution. Gastrointest Endosc. 2006;64:52–59. - PubMed
-
- Maranki J, Hernandez A J, Arslan B et al.Interventional endoscopic ultrasound-guided cholangiography: long-term experience of an emerging alternative to percutaneous transhepatic cholangiography. Endoscopy. 2009;41:532–538. - PubMed
-
- Kim Y S, Gupta K, Mallery S et al.Endoscopic ultrasound rendezvous for bile duct access using a transduodenal approach: cumulative experience at a single center. A case series. Endoscopy. 2010;42:496–502. - PubMed
-
- Fabbri C, Luigiano C, Fuccio L et al.EUS-guided biliary drainage with placement of a new partially covered biliary stent for palliation of malignant biliary obstruction: a case series. Endoscopy. 2011;43:438–441. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical