

Intracoronary Imaging in the Detection of Vulnerable Plaques
- PMID: 26879196
- PMCID: PMC4754333
- DOI: 10.1007/s11886-016-0705-1
Intracoronary Imaging in the Detection of Vulnerable Plaques
Abstract
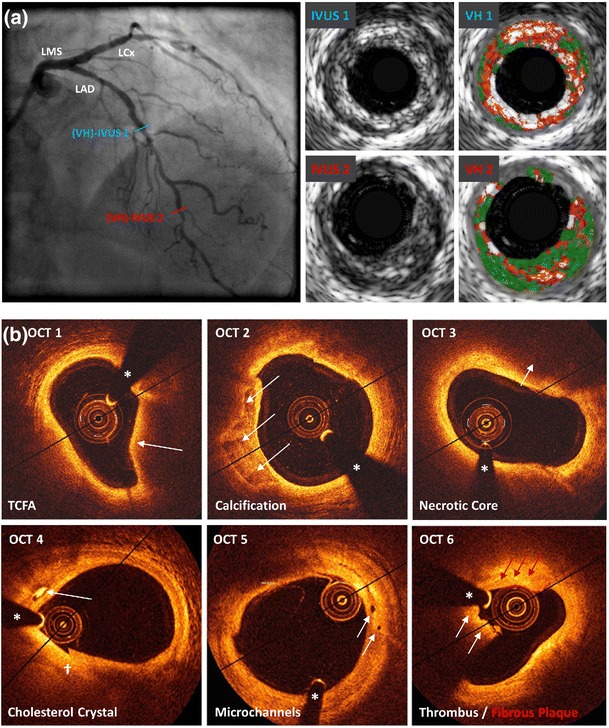
Coronary artery disease is the result of atherosclerotic changes to the coronary arterial wall, comprising endothelial dysfunction, vascular inflammation and deposition of lipid-rich macrophage foam cells. Certain high-risk atherosclerotic plaques are vulnerable to disruption, leading to rupture, thrombosis and the clinical sequelae of acute coronary syndrome. Though recognised as the gold standard for evaluating the presence, distribution and severity of atherosclerotic lesions, invasive coronary angiography is incapable of identifying non-stenotic, vulnerable plaques that are responsible for adverse cardiovascular events. The recognition of such limitations has impelled the development of intracoronary imaging technologies, including intravascular ultrasound, optical coherence tomography and near-infrared spectroscopy, which enable the detailed evaluation of the coronary wall and atherosclerotic plaques in clinical practice. This review discusses the present status of invasive imaging technologies; summarises up-to-date, evidence-based clinical guidelines; and addresses questions that remain unanswered with regard to the future of intracoronary plaque imaging.
Keywords: Coronary artery disease; Imaging; Interventional cardiology; Intravascular ultrasonography; Near-infrared spectroscopy; Optical coherence tomography.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
