

Pentraxin-3 as a marker of disease severity and risk of death in patients with necrotizing soft tissue infections: a nationwide, prospective, observational study
- PMID: 26880104
- PMCID: PMC4754810
- DOI: 10.1186/s13054-016-1210-z
Pentraxin-3 as a marker of disease severity and risk of death in patients with necrotizing soft tissue infections: a nationwide, prospective, observational study
Abstract
Background: New biomarkers are needed to assess the severity of necrotizing soft tissue infection (NSTI) at an early stage and to individualize treatment strategies. We assessed pentraxin-3 (PTX3) as a marker of disease severity and risk of death in patients with NSTI.
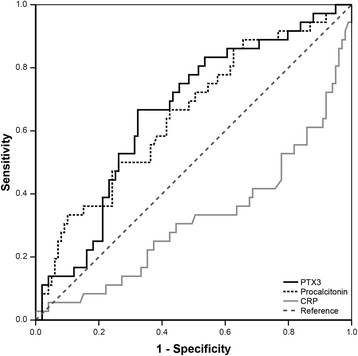
Methods: We conducted a prospective, observational study in the intensive care unit at Copenhagen University Hospital, where treatment of NSTI is centralized at a national level. We compared PTX3, procalcitonin and C-reactive protein in septic shock versus nonshock patients and in amputated versus nonamputated patients using the Mann-Whitney U test. The prognostic value of the markers for 180-day mortality was assessed using Cox regression analyses.
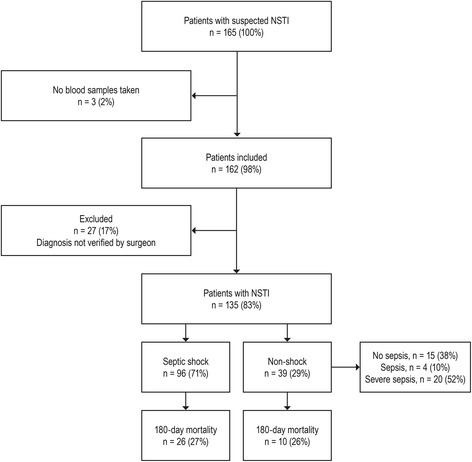
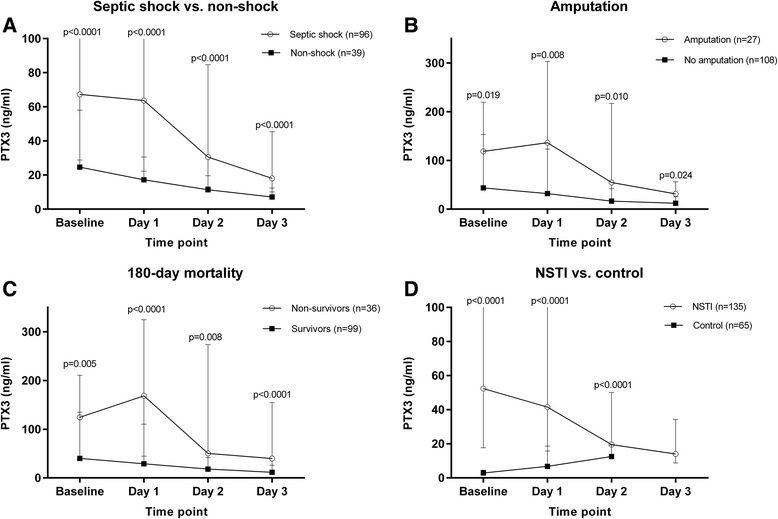
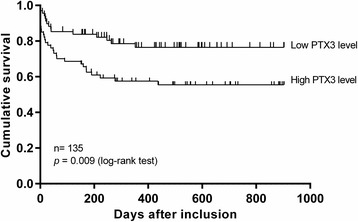
Results: Patients with NSTI (n = 135) were included over 25 months with up to 2.5-year follow-up; 71% had septic shock, amputation was undertaken in 20% and the 180-day mortality was 27%. Baseline plasma PTX3 level was significantly higher in patients with septic shock (67.3 versus 24.6 ng/mL, p < 0.0001) and in patients who underwent amputation (118.6 versus 43.6 ng/mL, p = 0.019). No significant differences in baseline procalcitonin or C-reactive protein levels were found according to amputation (25.2 versus 7.0 μg/L, p = 0.060 and 202 versus 225 mg/L, p = 0.123), respectively. Baseline PTX3 level above the median was associated with death (p = 0.009, log-rank test) and the univariate Cox regression analysis revealed a significant association between PTX3 level upon admission and 180-day mortality (hazard ratio 2.60 (95% confidence interval 1.28-5.29), p = 0.008). When adjusted for age, sex, chronic disease and Simplified Acute Physiology Score II, no significant association was found.
Conclusions: High PTX3 level is associated with septic shock, amputation and risk of death in patients with NSTI, but it is not an independent predictor of 180-day mortality in this patient group.
Trial registration: ClinicalTrials.gov Identifier: NCT02180906. Date of registration: June 29, 2014.
Figures
Comment in
-
Pentraxin-3 to better delineate necrotizing soft tissue infection: not really!Crit Care. 2016 Jun 17;20(1):173. doi: 10.1186/s13054-016-1319-0. Crit Care. 2016. PMID: 27311489 Free PMC article. No abstract available.
References
-
- Bilton BD, Zibari GB, McMillan RW, Aultman DF, Dunn G, McDonald JC. Aggressive surgical management of necrotizing fasciitis serves to decrease mortality: a retrospective study. Am Surg. 1998;64:397–400. - PubMed
-
- Wong C-H, Chang H-C, Pasupathy S, Khin L-W, Tan J-L, Low C-O. Necrotizing fasciitis: clinical presentation, microbiology, and determinants of mortality. J Bone Joint Surg Am. 2003;85-A:1454–60. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
