

Impact of Awareness and Patterns of Nonhospitalized Atrial Fibrillation on the Risk of Mortality: The Reasons for Geographic And Racial Differences in Stroke (REGARDS) Study
- PMID: 26880475
- PMCID: PMC4769105
- DOI: 10.1002/clc.22501
Impact of Awareness and Patterns of Nonhospitalized Atrial Fibrillation on the Risk of Mortality: The Reasons for Geographic And Racial Differences in Stroke (REGARDS) Study
Abstract
Background: Although mortality associated with atrial fibrillation (AF) has been reported to decrease over prior decades, the mortality risk of asymptomatic, nonhospitalized AF has not been examined.
Hypothesis: Asymptomatic, nonhospitalized AF is associated with an increased risk of death.
Methods: This analysis included 25,976 participants (mean age, 65 ± 9.4 years; 55% female; 38% black) from the Reasons for Geographic And Racial Differences (REGARDS) study. Atrial fibrillation was detected on the baseline electrocardiogram (ECG AF) or by self-reported history. Atrial fibrillation unawareness was defined as present if ECG evidence of the arrhythmia was detected but no self-reported history was reported. All-cause mortality was confirmed during follow-up through March 31, 2014.
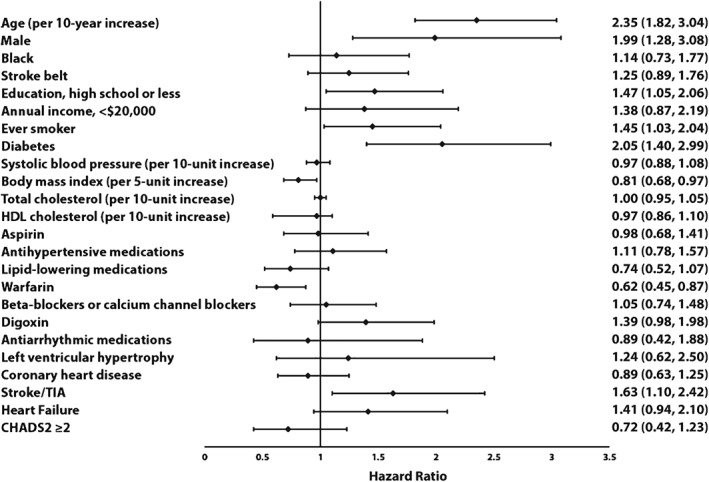
Results: A total of 2208 (8.5%) participants had AF at baseline (ECG: n = 371/17%; self-reported: n = 1837/83%). Over a median follow-up of 7.6 years, 3481 deaths occurred. In a multivariable Cox regression model, AF was associated with a 32% increased risk of mortality (95% confidence interval [CI]: 1.19-1.46). Risk of death was higher among those with ECG AF (hazard ratio: 1.71, 95% CI: 1.42-2.07) compared with self-reported cases (hazard ratio: 1.15, 95% CI: 1.03-1.29). Those who were unaware of their AF diagnosis had a 94% increased risk of death (95% CI: 1.50-2.52) compared with AF participants who were aware of their diagnosis.
Conclusions: Asymptomatic, nonhospitalized AF is associated with an increased risk of mortality in the general population. Mortality is higher in those with ECG-confirmed cases and among those who are unaware of their diagnosis.
© 2016 Wiley Periodicals, Inc.
Figures


Similar articles
-
Atrial fibrillation and incident end-stage renal disease: The REasons for Geographic And Racial Differences in Stroke (REGARDS) study.Int J Cardiol. 2015 Apr 15;185:219-23. doi: 10.1016/j.ijcard.2015.03.104. Epub 2015 Mar 12. Int J Cardiol. 2015. PMID: 25797681 Free PMC article.
-
Peripheral arterial disease and risk of atrial fibrillation and stroke: the Multi-Ethnic Study of Atherosclerosis.J Am Heart Assoc. 2014 Nov 17;3(6):e001270. doi: 10.1161/JAHA.114.001270. J Am Heart Assoc. 2014. PMID: 25404190 Free PMC article.
-
Association between Atrial Fibrillation and Three-Year Mortality in Nondiabetic Patients with Acute First-Ever Ischemic Stroke.J Stroke Cerebrovasc Dis. 2016 Nov;25(11):2660-2667. doi: 10.1016/j.jstrokecerebrovasdis.2016.07.012. Epub 2016 Jul 29. J Stroke Cerebrovasc Dis. 2016. PMID: 27480821
-
Atrial fibrillation and silent stroke: links, risks, and challenges.Vasc Health Risk Manag. 2016 Mar 7;12:65-74. doi: 10.2147/VHRM.S81807. eCollection 2016. Vasc Health Risk Manag. 2016. PMID: 27022272 Free PMC article. Review.
-
Atrial fibrillation and stroke. Mortality and causes of death after the first acute ischemic stroke.Stroke. 1997 Feb;28(2):311-5. doi: 10.1161/01.str.28.2.311. Stroke. 1997. PMID: 9040681 Review.
Cited by
-
The appropriate use of risk scores in the prediction of atrial fibrillation.J Thorac Dis. 2016 Oct;8(10):E1391-E1394. doi: 10.21037/jtd.2016.10.96. J Thorac Dis. 2016. PMID: 27867638 Free PMC article. No abstract available.
-
Atrial fibrillation in Black American patients: A review of genetics, risk factors, and outcomes.Heart Rhythm. 2025 Mar;22(3):617-626. doi: 10.1016/j.hrthm.2024.10.074. Epub 2024 Nov 6. Heart Rhythm. 2025. PMID: 39515500 Review.
-
Older Adults at Risk for Atrial Fibrillation Lack Knowledge and Confidence to Seek Treatment for Signs and Symptoms.SAGE Open Nurs. 2017 Jan-Dec;3:10.1177/2377960817720324. doi: 10.1177/2377960817720324. Epub 2017 Aug 29. SAGE Open Nurs. 2017. PMID: 30637335 Free PMC article.
-
Association of chronic kidney disease with all-cause mortality in patients hospitalized for atrial fibrillation and impact of clinical and socioeconomic factors on this association.Front Cardiovasc Med. 2022 Nov 24;9:945106. doi: 10.3389/fcvm.2022.945106. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 36505361 Free PMC article.
-
Racial and Ethnic Considerations in Patients With Atrial Fibrillation: JACC Focus Seminar 5/9.J Am Coll Cardiol. 2021 Dec 21;78(25):2563-2572. doi: 10.1016/j.jacc.2021.04.110. J Am Coll Cardiol. 2021. PMID: 34887142 Free PMC article. Review.
References
-
- Go AS, Hylek EM, Phillips KA, et al. Prevalence of diagnosed atrial fibrillation in adults: national implications for rhythm management and stroke prevention: the AnTicoagulation and Risk Factors in Atrial Fibrillation (ATRIA) Study. JAMA. 2001;285:2370–2375. - PubMed
-
- Benjamin EJ, Levy D, Vaziri SM, et al. Independent risk factors for atrial fibrillation in a population‐based cohort: the Framingham Heart Study. JAMA. 1994;271:840–844. - PubMed
-
- Heeringa J, Kors JA, Hofman A, et al. Cigarette smoking and risk of atrial fibrillation: the Rotterdam Study. Am Heart J. 2008;156:1163–1169. - PubMed
-
- Wolf PA, Abbott RD, Kannel WB. Atrial fibrillation as an independent risk factor for stroke: the Framingham Study. Stroke. 1991;22:983–988. - PubMed
-
- Gottdiener JS, Arnold AM, Aurigemma GP, et al. Predictors of congestive heart failure in the elderly: the Cardiovascular Health Study. J Am Coll Cardiol. 2000;35:1628–1637. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
