

Association Between Interstitial Lung Abnormalities and All-Cause Mortality
- PMID: 26881370
- PMCID: PMC4828973
- DOI: 10.1001/jama.2016.0518
Association Between Interstitial Lung Abnormalities and All-Cause Mortality
Abstract
Importance: Interstitial lung abnormalities have been associated with lower 6-minute walk distance, diffusion capacity for carbon monoxide, and total lung capacity. However, to our knowledge, an association with mortality has not been previously investigated.
Objective: To investigate whether interstitial lung abnormalities are associated with increased mortality.
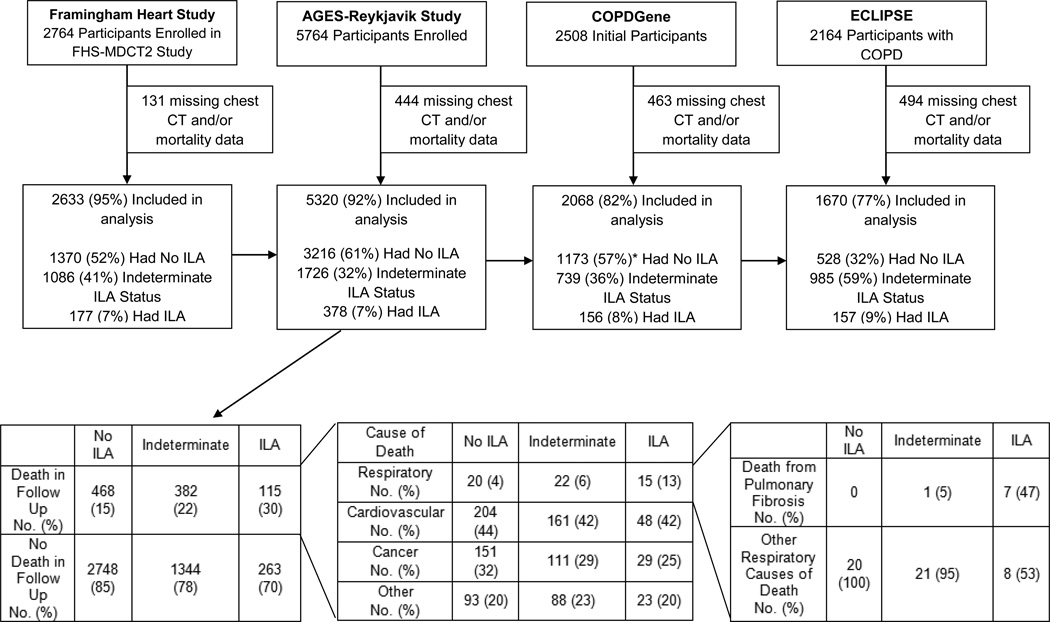
Design, setting, and population: Prospective cohort studies of 2633 participants from the FHS (Framingham Heart Study; computed tomographic [CT] scans obtained September 2008-March 2011), 5320 from the AGES-Reykjavik Study (Age Gene/Environment Susceptibility; recruited January 2002-February 2006), 2068 from the COPDGene Study (Chronic Obstructive Pulmonary Disease; recruited November 2007-April 2010), and 1670 from ECLIPSE (Evaluation of COPD Longitudinally to Identify Predictive Surrogate Endpoints; between December 2005-December 2006).
Exposures: Interstitial lung abnormality status as determined by chest CT evaluation.
Main outcomes and measures: All-cause mortality over an approximate 3- to 9-year median follow-up time. Cause-of-death information was also examined in the AGES-Reykjavik cohort.
Results: Interstitial lung abnormalities were present in 177 (7%) of the 2633 participants from FHS, 378 (7%) of 5320 from AGES-Reykjavik, 156 (8%) of 2068 from COPDGene, and in 157 (9%) of 1670 from ECLIPSE. Over median follow-up times of approximately 3 to 9 years, there were more deaths (and a greater absolute rate of mortality) among participants with interstitial lung abnormalities when compared with those who did not have interstitial lung abnormalities in the following cohorts: 7% vs 1% in FHS (6% difference [95% CI, 2% to 10%]), 56% vs 33% in AGES-Reykjavik (23% difference [95% CI, 18% to 28%]), and 11% vs 5% in ECLIPSE (6% difference [95% CI, 1% to 11%]). After adjustment for covariates, interstitial lung abnormalities were associated with a higher risk of death in the FHS (hazard ratio [HR], 2.7 [95% CI, 1.1 to 6.5]; P = .03), AGES-Reykjavik (HR, 1.3 [95% CI, 1.2 to 1.4]; P < .001), COPDGene (HR, 1.8 [95% CI, 1.1 to 2.8]; P = .01), and ECLIPSE (HR, 1.4 [95% CI, 1.1 to 2.0]; P = .02) cohorts. In the AGES-Reykjavik cohort, the higher rate of mortality could be explained by a higher rate of death due to respiratory disease, specifically pulmonary fibrosis.
Conclusions and relevance: In 4 separate research cohorts, interstitial lung abnormalities were associated with a greater risk of all-cause mortality. The clinical implications of this association require further investigation.
Trial registration: ClinicalTrials.gov NCT00292552.
Conflict of interest statement
No other disclosures are reported.
Figures


Comment in
-
Interstitial lung abnormalities are linked to increased risk of death.BMJ. 2016 Feb 16;352:i971. doi: 10.1136/bmj.i971. BMJ. 2016. PMID: 26888662 No abstract available.
References
-
- Sverzellati N, Guerci L, Randi G, et al. Interstitial lung diseases in a lung cancer screening trial. Eur Respir J. 2011;38:392–400. - PubMed
-
- Tsushima K, Sone S, Yoshikawa S, Yokoyama T, Suzuki T, Kubo K. The radiological patterns of interstitial change at an early phase: over a 4-year follow-up. Respir Med. 2010;104:1712–1721. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
- 27120120022C/PHS HHS/United States
- 1K23CA157631/CA/NCI NIH HHS/United States
- U01 HL089897/HL/NHLBI NIH HHS/United States
- R01 HL116931/HL/NHLBI NIH HHS/United States
- R01 HL116473/HL/NHLBI NIH HHS/United States
- R01 HL107246/HL/NHLBI NIH HHS/United States
- K25 HL104085/HL/NHLBI NIH HHS/United States
- K23 CA157631/CA/NCI NIH HHS/United States
- P01 HL114501/HL/NHLBI NIH HHS/United States
- R01 HL113264/HL/NHLBI NIH HHS/United States
- N01-HC-25195/HC/NHLBI NIH HHS/United States
- R01 HL122464/HL/NHLBI NIH HHS/United States
- R01 HL089897/HL/NHLBI NIH HHS/United States
- T32 HL007633/HL/NHLBI NIH HHS/United States
- S10 OD018526/OD/NIH HHS/United States
- K08 HL097029/HL/NHLBI NIH HHS/United States
- R01 HL130974/HL/NHLBI NIH HHS/United States
- R01 HL089856/HL/NHLBI NIH HHS/United States
- N01-AG-1-2100/AG/NIA NIH HHS/United States
- K01 HL118714/HL/NHLBI NIH HHS/United States
- R01 HL111024/HL/NHLBI NIH HHS/United States
- U01 HL089856/HL/NHLBI NIH HHS/United States
- HHSN27120120022C/PHS HHS/United States
- ImNIH/Intramural NIH HHS/United States
- N01 HC025195/HL/NHLBI NIH HHS/United States
- R21 HL119902/HL/NHLBI NIH HHS/United States
- P01 HL105339/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
