

Computational pathology of pre-treatment biopsies identifies lymphocyte density as a predictor of response to neoadjuvant chemotherapy in breast cancer
- PMID: 26882907
- PMCID: PMC4755003
- DOI: 10.1186/s13058-016-0682-8
Computational pathology of pre-treatment biopsies identifies lymphocyte density as a predictor of response to neoadjuvant chemotherapy in breast cancer
Abstract
Background: There is a need to improve prediction of response to chemotherapy in breast cancer in order to improve clinical management and this may be achieved by harnessing computational metrics of tissue pathology. We investigated the association between quantitative image metrics derived from computational analysis of digital pathology slides and response to chemotherapy in women with breast cancer who received neoadjuvant chemotherapy.
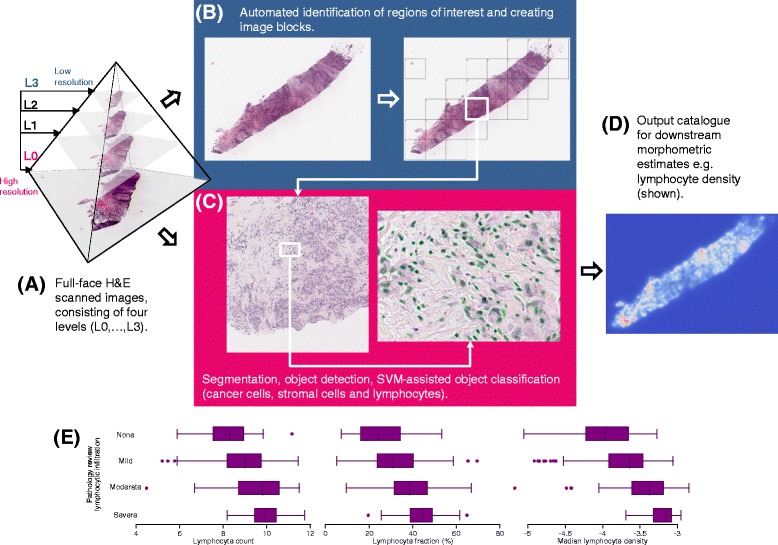
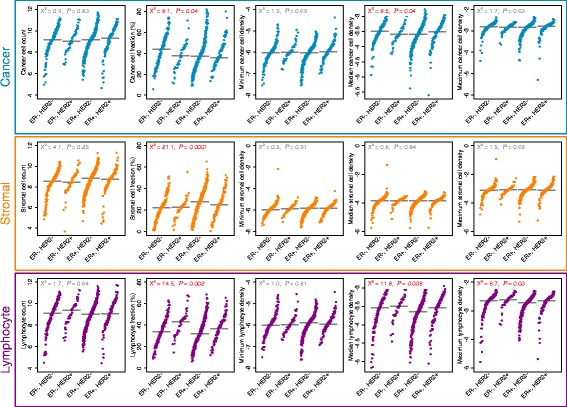
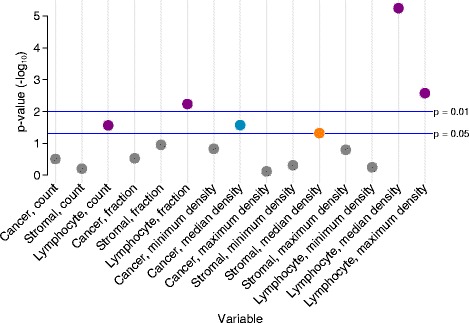
Methods: We digitised tissue sections of both diagnostic and surgical samples of breast tumours from 768 patients enrolled in the Neo-tAnGo randomized controlled trial. We subjected digital images to systematic analysis optimised for detection of single cells. Machine-learning methods were used to classify cells as cancer, stromal or lymphocyte and we computed estimates of absolute numbers, relative fractions and cell densities using these data. Pathological complete response (pCR), a histological indicator of chemotherapy response, was the primary endpoint. Fifteen image metrics were tested for their association with pCR using univariate and multivariate logistic regression.
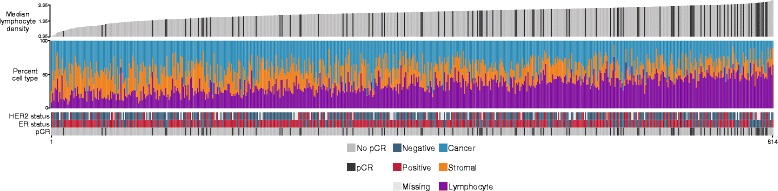
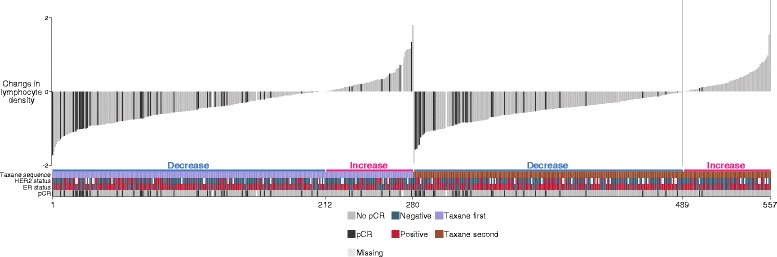
Results: Median lymphocyte density proved most strongly associated with pCR on univariate analysis (OR 4.46, 95 % CI 2.34-8.50, p < 0.0001; observations = 614) and on multivariate analysis (OR 2.42, 95 % CI 1.08-5.40, p = 0.03; observations = 406) after adjustment for clinical factors. Further exploratory analyses revealed that in approximately one quarter of cases there was an increase in lymphocyte density in the tumour removed at surgery compared to diagnostic biopsies. A reduction in lymphocyte density at surgery was strongly associated with pCR (OR 0.28, 95 % CI 0.17-0.47, p < 0.0001; observations = 553).
Conclusions: A data-driven analysis of computational pathology reveals lymphocyte density as an independent predictor of pCR. Paradoxically an increase in lymphocyte density, following exposure to chemotherapy, is associated with a lack of pCR. Computational pathology can provide objective, quantitative and reproducible tissue metrics and represents a viable means of outcome prediction in breast cancer.
Trial registration: ClinicalTrials.gov NCT00070278 ; 03/10/2003.
Figures
References
-
- Berruti A, Amoroso V, Gallo F, Bertaglia V, Simoncini E, Pedersini R, et al. Pathologic complete response as a potential surrogate for the clinical outcome in patients with breast cancer after neoadjuvant therapy: a meta-regression of 29 randomized prospective studies. J Clin Oncol. 2014;32(34):3883–91. doi: 10.1200/JCO.2014.55.2836. - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
