

Adaptive resistance to therapeutic PD-1 blockade is associated with upregulation of alternative immune checkpoints
- PMID: 26883990
- PMCID: PMC4757784
- DOI: 10.1038/ncomms10501
Adaptive resistance to therapeutic PD-1 blockade is associated with upregulation of alternative immune checkpoints
Abstract
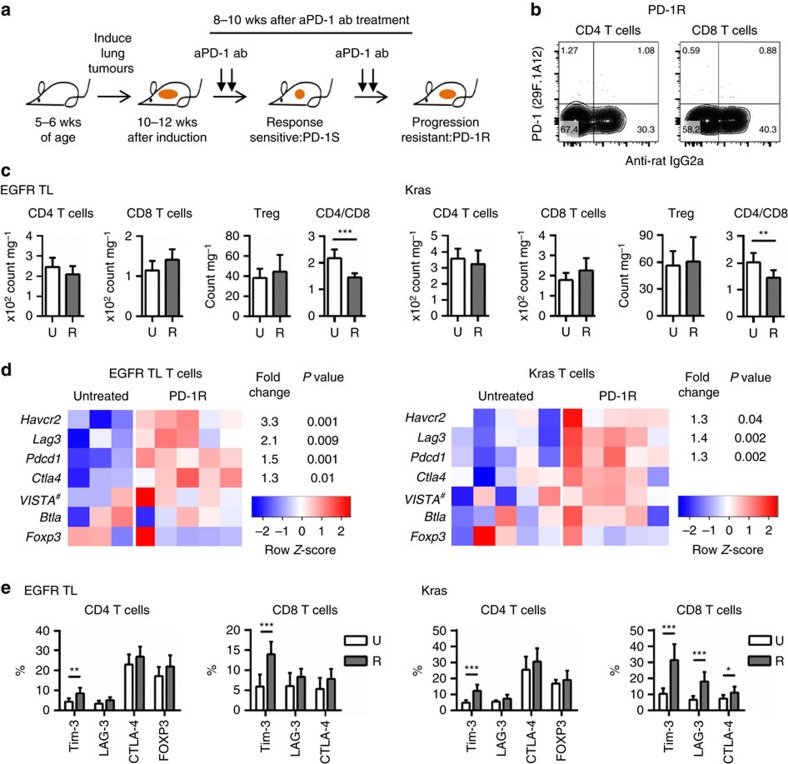
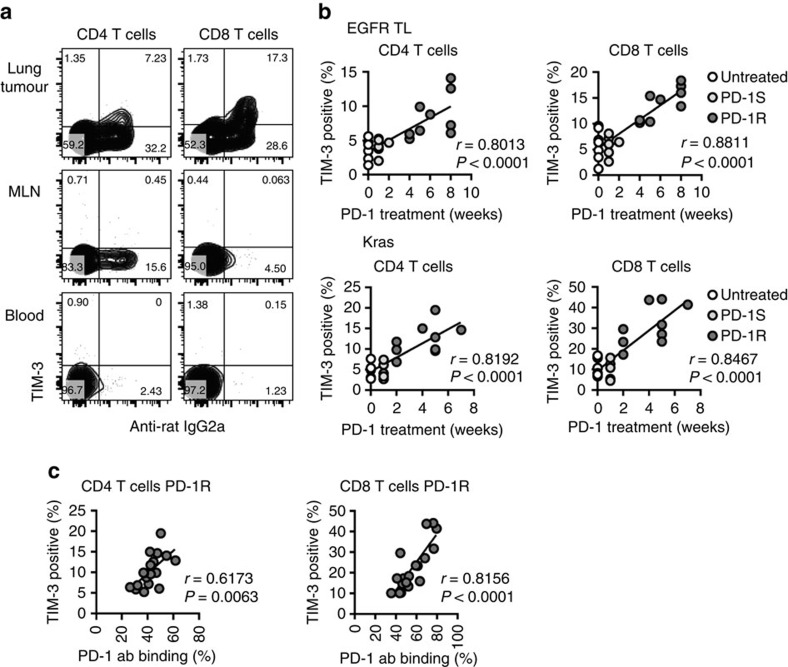
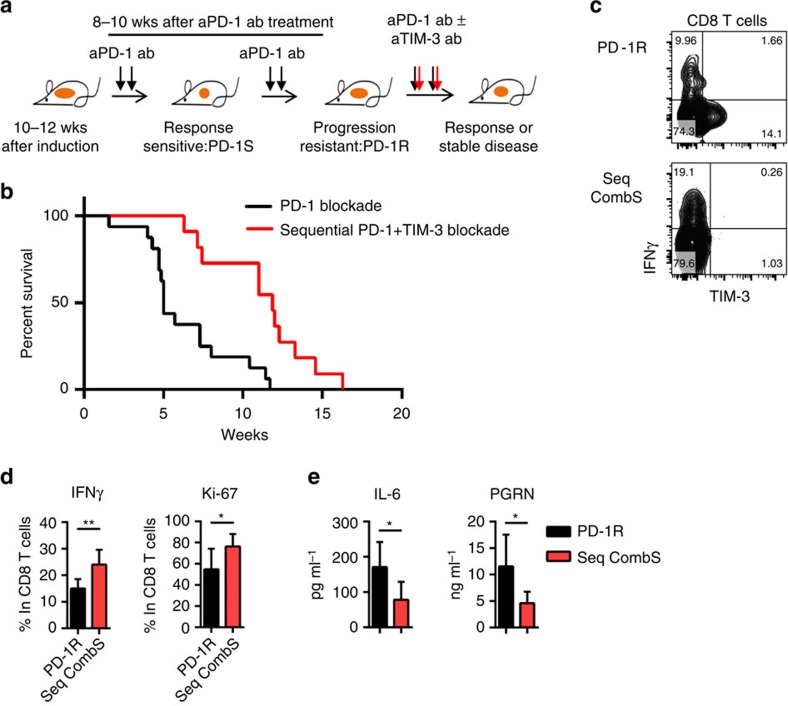
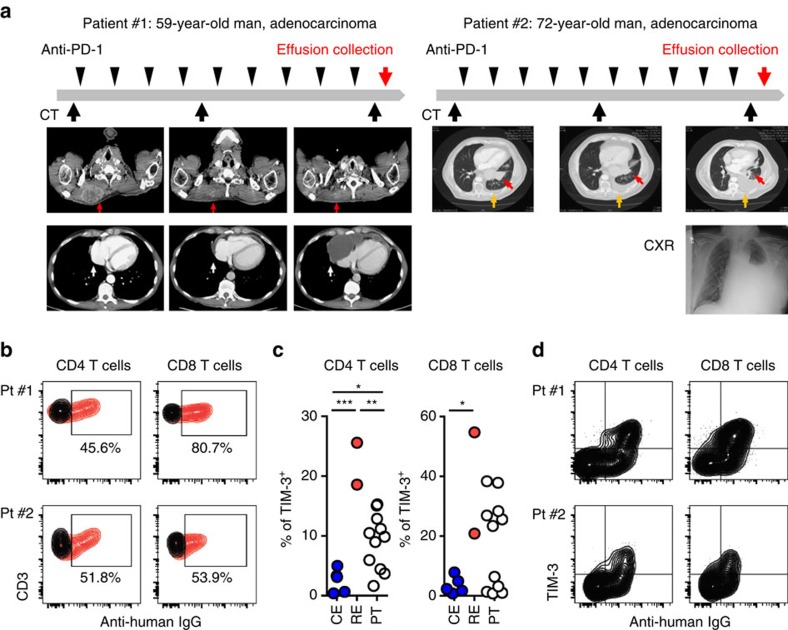
Despite compelling antitumour activity of antibodies targeting the programmed death 1 (PD-1): programmed death ligand 1 (PD-L1) immune checkpoint in lung cancer, resistance to these therapies has increasingly been observed. In this study, to elucidate mechanisms of adaptive resistance, we analyse the tumour immune microenvironment in the context of anti-PD-1 therapy in two fully immunocompetent mouse models of lung adenocarcinoma. In tumours progressing following response to anti-PD-1 therapy, we observe upregulation of alternative immune checkpoints, notably T-cell immunoglobulin mucin-3 (TIM-3), in PD-1 antibody bound T cells and demonstrate a survival advantage with addition of a TIM-3 blocking antibody following failure of PD-1 blockade. Two patients who developed adaptive resistance to anti-PD-1 treatment also show a similar TIM-3 upregulation in blocking antibody-bound T cells at treatment failure. These data suggest that upregulation of TIM-3 and other immune checkpoints may be targetable biomarkers associated with adaptive resistance to PD-1 blockade.
Conflict of interest statement
G.D. received sponsored research support from Bristol-Myers Squibb and Novartis. He is currently an employee of Novartis. F.S.H. is a Bristol-Myers Squibb nonpaid consultant, Novartis, Merck and Genentech consultant and receives clinical trial support to the institution from these companies. G.J.F. receives patent royalties on the PD-1 pathway from Bristol-Myers-Squibb, Roche, Merck, EMD-Serrono, Boehringer-Ingelheim, Amplimmune/AstraZeneca and Novartis and patent royalties on the TIM-3 pathway from Novartis. D.B.C. is a consultant for Pfizer. S.J.R. receives research support from Bristol-Myers Squibb and the Center for Immune Oncology, DFCI. The remaining authors declare no competing financial interests.
Figures
Comment in
-
Immunotherapy: PD-1 says goodbye, TIM-3 says hello.Nat Rev Clin Oncol. 2016 Apr;13(4):202-3. doi: 10.1038/nrclinonc.2016.40. Epub 2016 Mar 15. Nat Rev Clin Oncol. 2016. PMID: 26977783 No abstract available.
References
-
- Page D. B., Postow M. A., Callahan M. K., Allison J. P. & Wolchok J. D. Immune modulation in cancer with antibodies. Annu. Rev. Med. 65, 185–202 (2014). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- 5R01CA163896-04/CA/NCI NIH HHS/United States
- R01 CA205150/CA/NCI NIH HHS/United States
- CA090578/CA/NCI NIH HHS/United States
- R01 CA166480/CA/NCI NIH HHS/United States
- 1R01CA195740-01/CA/NCI NIH HHS/United States
- P01 CA120964/CA/NCI NIH HHS/United States
- 5R01CA122794-10/CA/NCI NIH HHS/United States
- R01 CA195754/CA/NCI NIH HHS/United States
- P20 CA090578/CA/NCI NIH HHS/United States
- R01 CA140594/CA/NCI NIH HHS/United States
- 5R01CA140594-07/CA/NCI NIH HHS/United States
- R01 CA163896/CA/NCI NIH HHS/United States
- 5R01CA166480-04/CA/NCI NIH HHS/United States
- R01 CA122794/CA/NCI NIH HHS/United States
- P50 CA090578/CA/NCI NIH HHS/United States
- R01AI08995/AI/NIAID NIH HHS/United States
- R01 CA195740/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
