

Extended Pneumocephalus after Drainage of Chronic Subdural Hematoma Associated with Intracranial Hypotension : Case Report with Pathophysiologic Consideration
- PMID: 26885290
- PMCID: PMC4754592
- DOI: 10.3340/jkns.2016.59.1.69
Extended Pneumocephalus after Drainage of Chronic Subdural Hematoma Associated with Intracranial Hypotension : Case Report with Pathophysiologic Consideration
Abstract
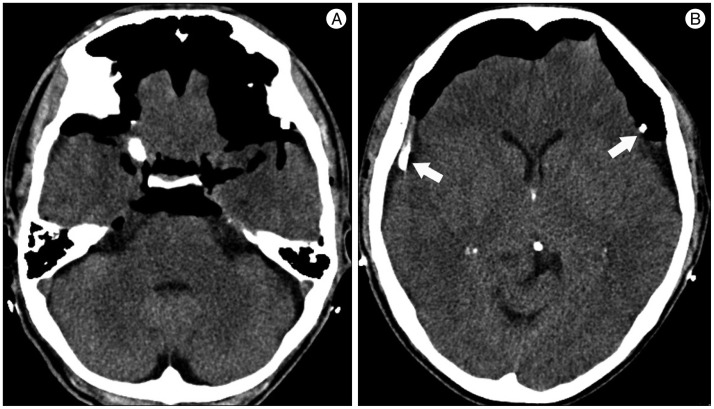
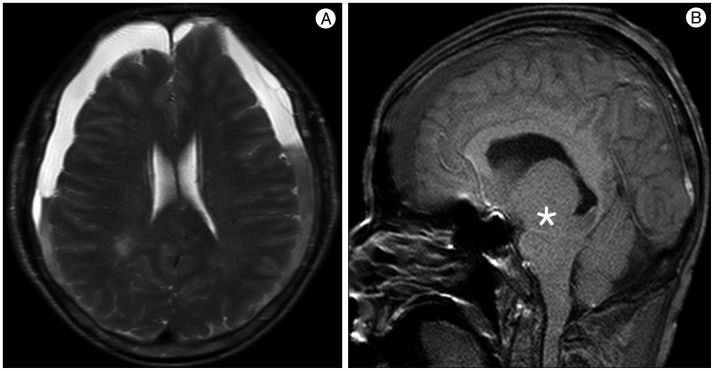
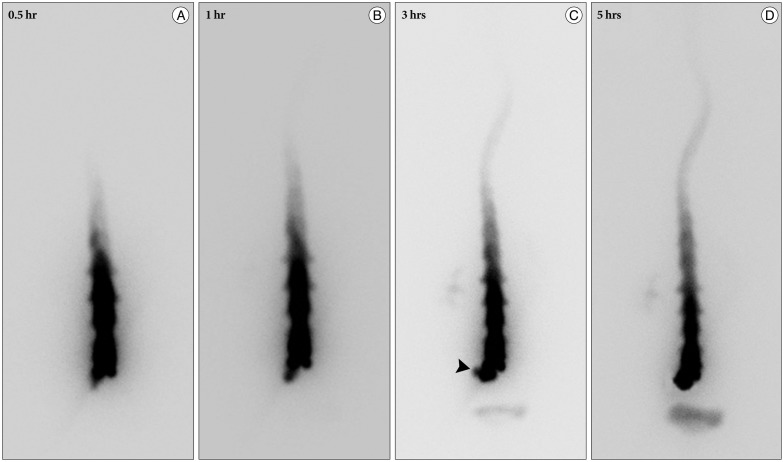
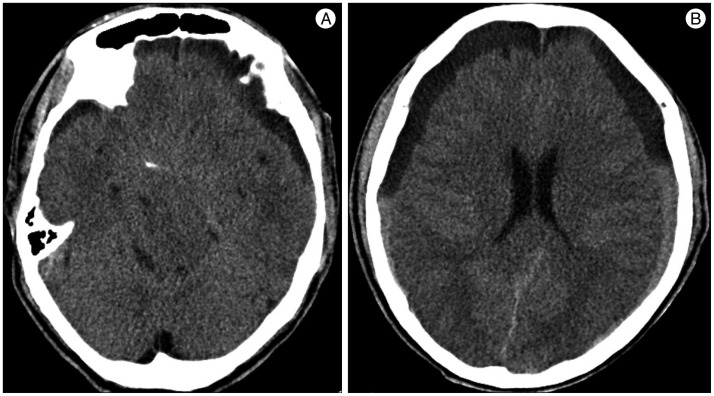
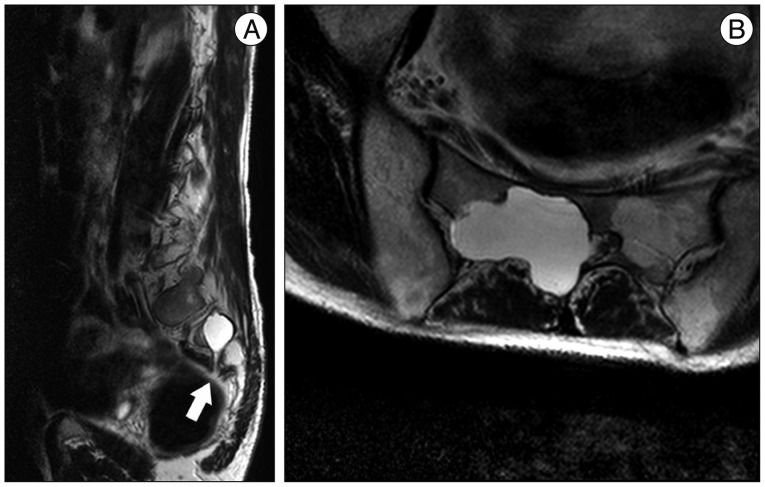
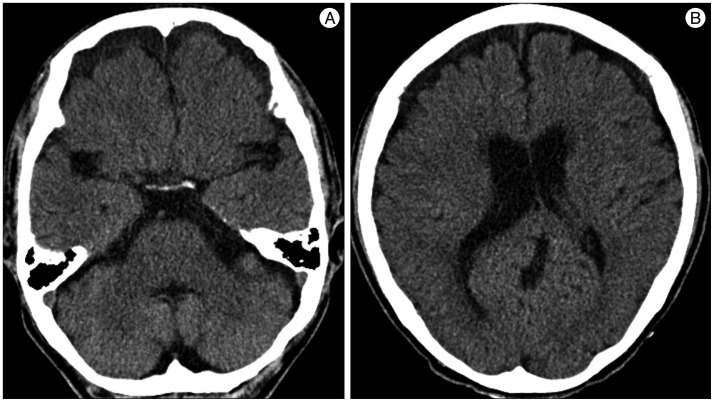
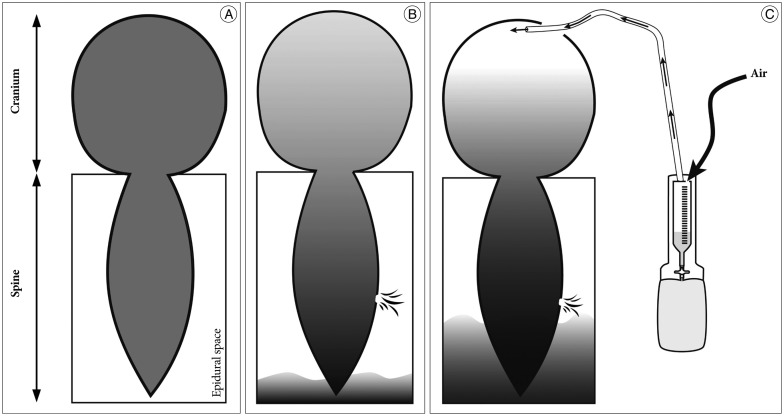
Chronic subdural hematoma (SDH) is a well-known disease entity and is traditionally managed with surgery. However, when associated with spontaneous intracranial hypotension (SIH), the treatment strategy ought to be modified, as classical treatment could lead to unwanted consequences. A 59-year-old man presented with a case of SIH that manifested as a bilateral chronic SDH. He developed fatal extensive pneumocephalus and SDH re-accumulation as a complication of burr-hole drainage. Despite application of an epidural blood patch, the spinal cerebrospinal fluid leak continued, which required open spinal surgery. Chronic SDH management should not be overlooked, especially if the exact cause has not been determined. When chronic SDH assumed to be associated with SIH, the neurosurgeon should determine the exact cause of SIH in order to effectively correct the cause.
Keywords: Chronic subdural hematoma; Intracranial hypotension; Pneumocephalus.
Figures

References
-
- Ducruet AF, Grobelny BT, Zacharia BE, Hickman ZL, DeRosa PL, Andersen KN, et al. The surgical management of chronic subdural hematoma. Neurosurg Rev. 2012;35:155–169. discussion 169. - PubMed
-
- Fishman RA, Dillon WP. Dural enhancement and cerebral displacement secondary to intracranial hypotension. Neurology. 1993;43(3 Pt 1):609–611. - PubMed
-
- García-Morales I, Porta-Etessam J, Galán L, Lagares A, Molina JA. Recurrent subdural haematomas in a patient with spontaneous intracranial hypotension. Cephalalgia. 2001;21:703–705. - PubMed
-
- Gordon N. Spontaneous intracranial hypotension. Dev Med Child Neurol. 2009;51:932–935. - PubMed
-
- Güler S, Çağlı B, Utku U, Ünlü E, Çelik Y. Intracranial hypotension is a rare cause of orthostatic headache : a review of the etiology, treatment and prognosis of 13 cases. Agri. 2013;25:69–77. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
