

Urinary sodium excretion predicts blood pressure response to spironolactone in patients with resistant hypertension independent of aldosterone status
- PMID: 26886564
- PMCID: PMC5636624
- DOI: 10.1097/HJH.0000000000000870
Urinary sodium excretion predicts blood pressure response to spironolactone in patients with resistant hypertension independent of aldosterone status
Abstract
Objective: Resistant hypertension (RHTN), blood pressure (BP) at least 140/90 mmHg despite using at least three different medications, including a diuretic, is associated with high dietary sodium and hyperaldosteronism. Mineralocorticoid receptor antagonists are recommended for treatment of RHTN, however, BP response to these agents varies widely. In the current analysis, we assessed predictors of BP response to spironolactone in patients with RHTN.
Methods: We retrospectively evaluated the BP response to adding spironolactone 12.5-25 mg to existing medications. A favorable BP response was defined as a reduction in SBP of at least 10 mmHg. Tested variables included baseline characteristics and biochemical parameters.
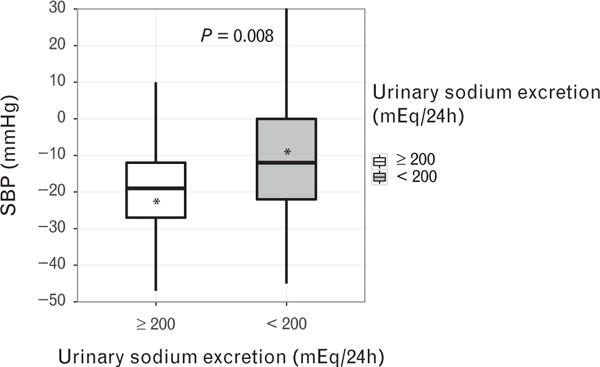
Results: A total of 79 patients with RHTN were included in the analysis. Evaluated patients were more likely women (53.2%) and African-American (55.8%); were generally obese (76%) and were prescribed an average of four antihypertensive medications. Baseline SBP was 153.6 ± 22.3 mmHg; addition of spironolactone resulted in a mean reduction of 15.5 ± 20.7 mmHg. Patients with high urinary sodium excretion (≥200 mEq/24 h) had a significantly greater BP reduction compared with patients with normal excretion (<200 mEq/24 h) (P = 0.008). Multivariable analysis identified 24 h urinary sodium excretion as a significant predictor of BP response (P = 0.021) after controlling for potential confounders, including primary aldosteronism.
Conclusion: The antihypertensive effect of spironolactone is positively related to urinary sodium excretion regardless of aldosterone status. These findings suggest that mineralocorticoid receptor antagonists may be of preferential benefit in counteracting the BP effects of high dietary sodium.
Conflict of interest statement
There are no conflicts of interest.
Figures
Comment in
-
Predictors of blood pressure response to spironolactone.J Hypertens. 2016 May;34(5):845-7. doi: 10.1097/HJH.0000000000000897. J Hypertens. 2016. PMID: 27027381 No abstract available.
Similar articles
-
Spironolactone and Resistant Hypertension in Heart Failure With Preserved Ejection Fraction.Am J Hypertens. 2018 Mar 10;31(4):407-414. doi: 10.1093/ajh/hpx210. Am J Hypertens. 2018. PMID: 29228101 Free PMC article. Clinical Trial.
-
Management of resistant hypertension: aldosterone antagonists or intensification of diuretic therapy?Nephrology (Carlton). 2015 Aug;20(8):567-71. doi: 10.1111/nep.12475. Nephrology (Carlton). 2015. PMID: 25818266
-
Raised aldosterone to renin ratio predicts antihypertensive efficacy of spironolactone: a prospective cohort follow-up study.Br J Clin Pharmacol. 1999 Nov;48(5):756-60. doi: 10.1046/j.1365-2125.1999.00070.x. Br J Clin Pharmacol. 1999. PMID: 10594479 Free PMC article. Clinical Trial.
-
Managing resistant hypertension: focus on mineralocorticoid-receptor antagonists.Vasc Health Risk Manag. 2017 Oct 16;13:403-411. doi: 10.2147/VHRM.S138599. eCollection 2017. Vasc Health Risk Manag. 2017. PMID: 29081661 Free PMC article. Review.
-
Treatment of Resistant and Refractory Hypertension.Circ Res. 2019 Mar 29;124(7):1061-1070. doi: 10.1161/CIRCRESAHA.118.312156. Circ Res. 2019. PMID: 30920924 Free PMC article. Review.
Cited by
-
Diagnosing and Managing Primary Aldosteronism in Hypertensive Patients: a Case-Based Approach.Curr Cardiol Rep. 2016 Oct;18(10):97. doi: 10.1007/s11886-016-0774-1. Curr Cardiol Rep. 2016. PMID: 27566330 Review.
-
Efficacy and safety of a low-sodium diet and spironolactone in patients with stage 1-3a chronic kidney disease: a pilot study.BMC Nephrol. 2022 Mar 5;23(1):95. doi: 10.1186/s12882-022-02711-z. BMC Nephrol. 2022. PMID: 35247964 Free PMC article. Clinical Trial.
-
Antihypertensive Effect of Long-Term Monotherapy with Esaxerenone in Patients with Essential Hypertension: Relationship Between Baseline Urinary Sodium Excretion and Its Antihypertensive Effect.Adv Ther. 2022 Oct;39(10):4779-4791. doi: 10.1007/s12325-022-02282-3. Epub 2022 Aug 17. Adv Ther. 2022. PMID: 35976603 Free PMC article.
-
Sex-specific responses to mineralocorticoid receptor antagonism in hypertensive African American males and females.Biol Sex Differ. 2019 May 9;10(1):24. doi: 10.1186/s13293-019-0238-6. Biol Sex Differ. 2019. PMID: 31072402 Free PMC article.
-
Should All Patients with Resistant Hypertension Receive Spironolactone?Curr Hypertens Rep. 2016 Nov;18(11):81. doi: 10.1007/s11906-016-0690-1. Curr Hypertens Rep. 2016. PMID: 27787836 Review.
References
-
- Calhoun DA, Jones D, Textor S, et al. Resistant hypertension: diagnosis, evaluation, and treatment. Circulation. 2008;117(25):e510–e526. - PubMed
-
- McAdam-Marx, Ye X, Sung JC, Brixner DI, Khaler KH. Results of a retrospective, observational pilot study using electronic medical records to assess the prevalence and characteristics of patients with resistant hypertension in the ambulatory care setting. Clin Ther. 2009;31:1116–1123. - PubMed
-
- Garg JP, Elliot WJ, Folker A, et al. Resistant hypertension revisited: a comparison of two university-based cohorts. Am J Hypertens. 2005;18:619–626. - PubMed
-
- Shimosawa T. Salt, the renin-angiotensin-aldosterone system and resistant hypertension. Hypertens Res. 2013;36:657–660. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
