

Tracheobronchial Involvement of Rosai-Dorfman Disease: Case Report and Review of the Literature
- PMID: 26886634
- PMCID: PMC4998634
- DOI: 10.1097/MD.0000000000002821
Tracheobronchial Involvement of Rosai-Dorfman Disease: Case Report and Review of the Literature
Abstract
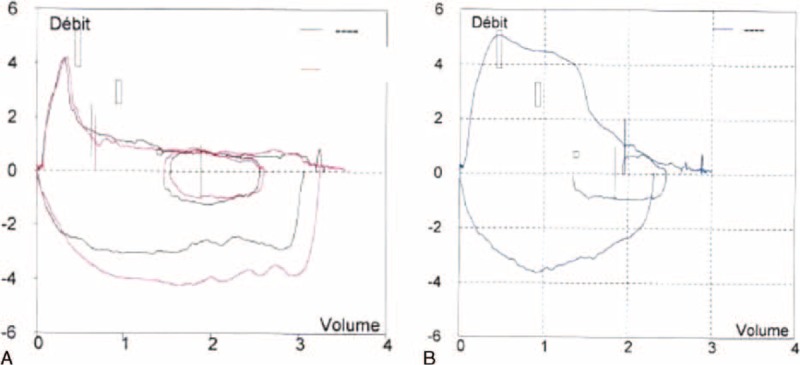
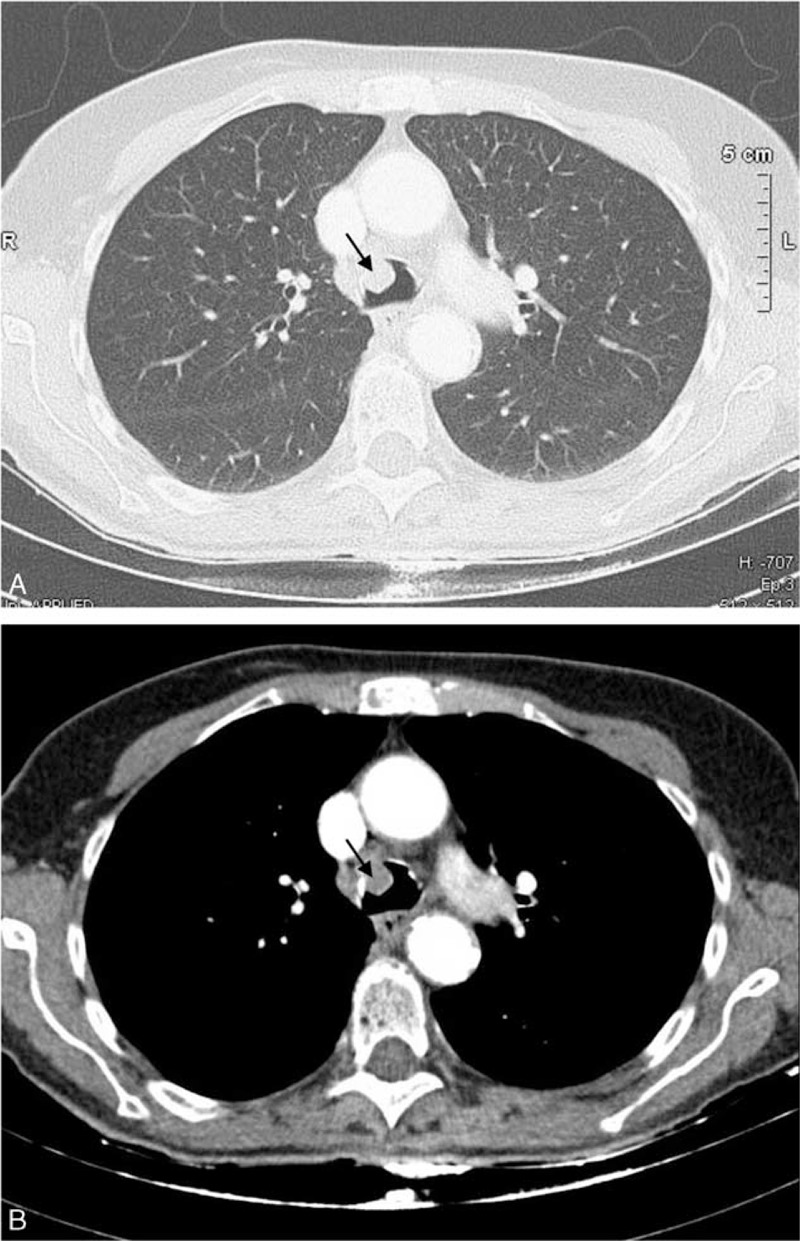
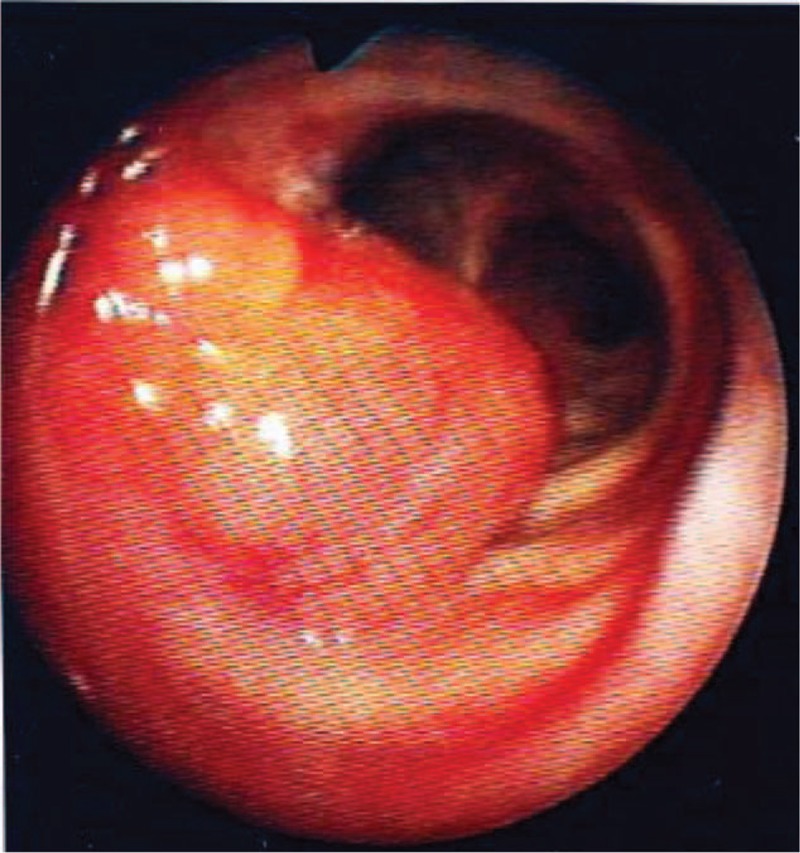
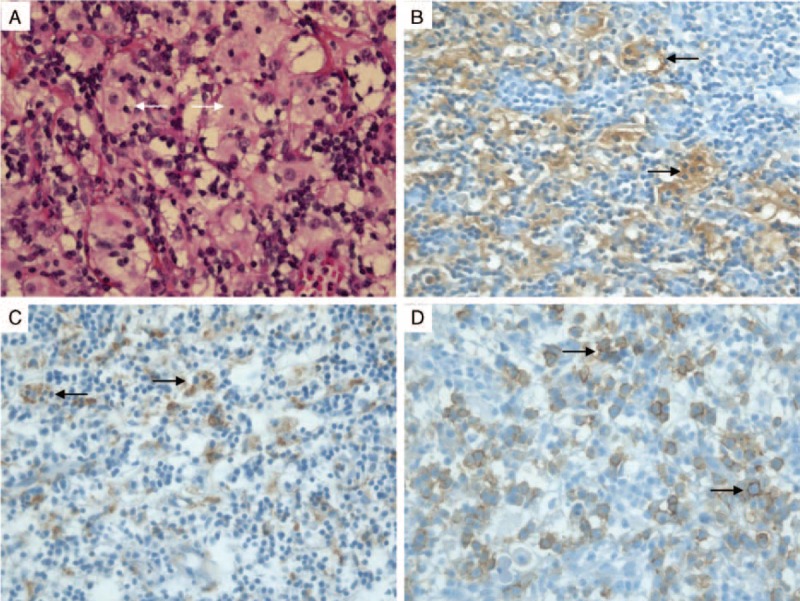
Rosai-Dorfman Disease (RDD) is a rare non-neoplastic entity, also known as sinus histiocytosis with massive lymphadenopathy (SHML), characterized by a benign proliferation of histiocytes in lymph nodes. Localized forms of RDD involving the tracheobronchial tree are very rare. There is no consensus regarding the management of central airway forms and recurrence is frequent. We report the case of an 81-year-old Caucasian woman admitted in 2014 for chronic cough. Her main medical past history included a diagnosis of sinonasal RDD in 1996 with recurrent obstructive rhinosinusitis requiring repeated sinonasal surgery, and a diagnosis of tracheal RDD in 2010 with 2 asymptomatic smooth lesions (5 and 7 mm) on the anterior tracheal wall. Physical examination was normal in 2014. Pulmonary function tests showed an obstructive pattern. Computed tomographic scan revealed a mass arising from the anterior wall of the trachea that projects into the tracheal lumen. Fiberoptic bronchoscopy showed a hypervascular multilobular lesion (2 cm) arising from the anterior tracheal wall and causing 50% obstruction of the tracheal lumen. Mechanical resection with electrocoagulation of the tracheal mass was performed by rigid bronchoscopy with no complication. Histological examination demonstrated tracheal RDD. One year after endotracheal resection, the patient presented no recurrence of cough and the obstructive pattern had resolved. Reports on tracheobronchial involvement are scarce. Symptomatic tracheobronchial obstruction requires mechanical resection by rigid bronchoscopy or surgery. Recurrence is frequent, justifying long-term follow-up.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Foucar E, Rosai J, Dorfman R. Sinus histiocytosis with massive lymphadenopathy (Rosai-Dorfman disease): review of the entity. Semin Diagn Pathol 1990; 7:19–73. - PubMed
-
- Cartin-Ceba R, Golbin JM, Yi ES, et al. Intrathoracic manifestations of Rosai-Dorfman disease. Respir Med 2010; 104:1344–1349. - PubMed
-
- Destombes P. Adenitis with lipid excess, in children or young adults, seen in the Antilles and in Mali (4 cases). Bull Société Pathol Exot Ses Fil 1965; 58:1169–1175. - PubMed
-
- Rosai J, Dorfman RF. Sinus histiocytosis with massive lymphadenopathy. A newly recognized benign clinicopathological entity. Arch Pathol 1969; 87:63–70. - PubMed
-
- Travis WDMD. Non-Neoplastic Disorders of the Lower Respiratory Tract. Vol 1. 1st ed2002; Washington, DC: Pathology AFI of American Registry of Pathology, 939.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
