

Safety and Efficacy of Solitaire Stent Thrombectomy: Individual Patient Data Meta-Analysis of Randomized Trials
- PMID: 26888532
- PMCID: PMC4760381
- DOI: 10.1161/STROKEAHA.115.012360
Safety and Efficacy of Solitaire Stent Thrombectomy: Individual Patient Data Meta-Analysis of Randomized Trials
Abstract
Background and purpose: Recent positive randomized trials of endovascular therapy for ischemic stroke used predominantly stent retrievers. We pooled data to investigate the efficacy and safety of stent thrombectomy using the Solitaire device in anterior circulation ischemic stroke.
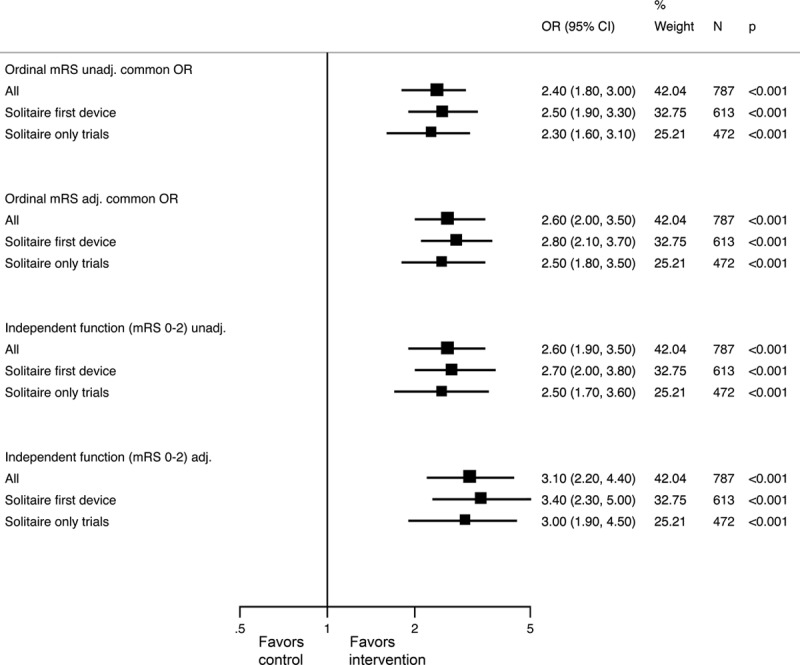
Methods: Patient-level data were pooled from trials in which the Solitaire was the only or the predominant device used in a prespecified meta-analysis (SEER Collaboration): Solitaire FR With the Intention for Thrombectomy as Primary Endovascular Treatment (SWIFT PRIME), Endovascular Treatment for Small Core and Anterior Circulation Proximal Occlusion With Emphasis on Minimizing CT to Recanalization Times (ESCAPE), Extending the Time for Thrombolysis in Emergency Neurological Deficits-Intra-Arterial (EXTEND-IA), and Randomized Trial of Revascularization With Solitaire FR Device Versus Best Medical Therapy in the Treatment of Acute Stroke Due to Anterior Circulation Large Vessel Occlusion Presenting Within Eight Hours of Symptom Onset (REVASCAT). The primary outcome was ordinal analysis of modified Rankin Score at 90 days. The primary analysis included all patients in the 4 trials with 2 sensitivity analyses: (1) excluding patients in whom Solitaire was not the first device used and (2) including the 3 Solitaire-only trials (excluding ESCAPE). Secondary outcomes included functional independence (modified Rankin Score 0-2), symptomatic intracerebral hemorrhage, and mortality.
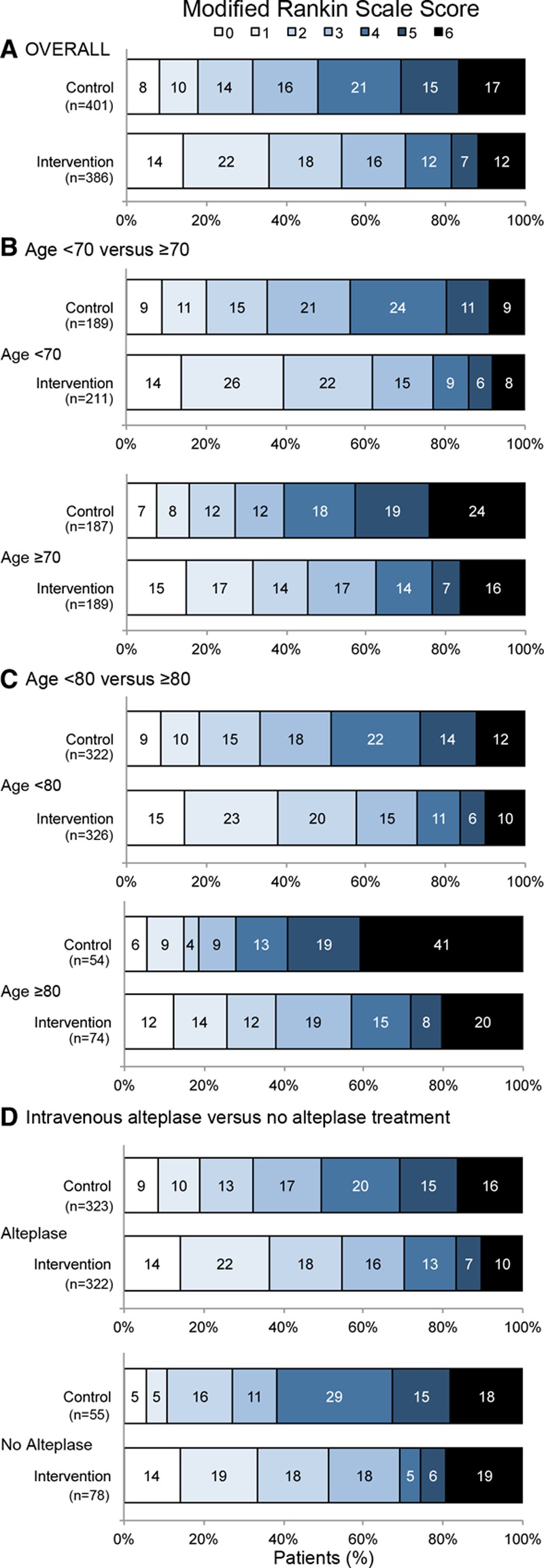
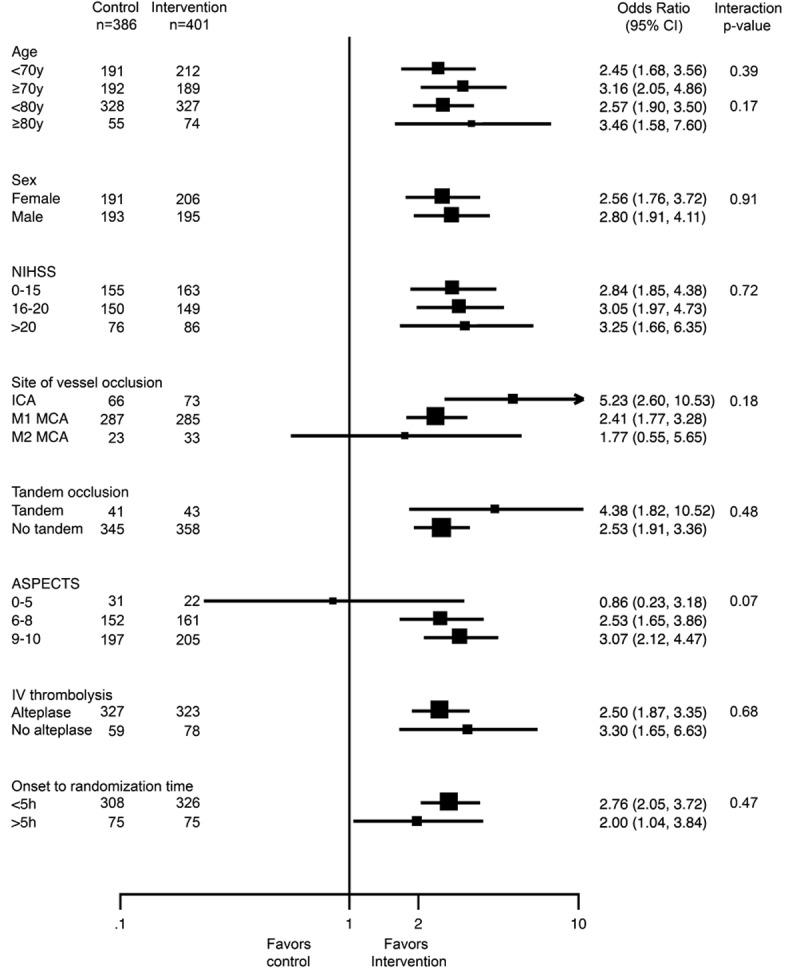
Results: The primary analysis included 787 patients: 401 randomized to endovascular thrombectomy and 386 to standard care, and 82.6% received intravenous thrombolysis. The common odds ratio for modified Rankin Score improvement was 2.7 (2.0-3.5) with no heterogeneity in effect by age, sex, baseline stroke severity, extent of computed tomography changes, site of occlusion, or pretreatment with alteplase. The number needed to treat to reduce disability was 2.5 and for an extra patient to achieve independent outcome was 4.25 (3.29-5.99). Successful revascularization occurred in 77% treated with Solitaire device. The rate of symptomatic intracerebral hemorrhage and overall mortality did not differ between treatment groups.
Conclusions: Solitaire thrombectomy for large vessel ischemic stroke was safe and highly effective with substantially reduced disability. Benefits were consistent in all prespecified subgroups.
Keywords: endovascular treatment; intra-arterial therapy; ischemic stroke; mechanical thrombectomy; meta-analysis; randomized controlled trial; stent retriever device; thrombolysis.
© 2016 The Authors.
Figures
References
-
- Berkhemer OA, Fransen PS, Beumer D, van den Berg LA, Lingsma HF, Yoo AJ, et al. MR CLEAN Investigators. A randomized trial of intraarterial treatment for acute ischemic stroke. N Engl J Med. 2015;372:11–20. doi: 10.1056/NEJMoa1411587. - PubMed
-
- Campbell BC, Mitchell PJ, Kleinig TJ, Dewey HM, Churilov L, Yassi N, et al. EXTEND-IA Investigators. Endovascular therapy for ischemic stroke with perfusion-imaging selection. N Engl J Med. 2015;372:1009–1018. doi: 10.1056/NEJMoa1414792. - PubMed
-
- Goyal M, Demchuk AM, Menon BK, Eesa M, Rempel JL, Thornton J, et al. ESCAPE Trial Investigators. Randomized assessment of rapid endovascular treatment of ischemic stroke. N Engl J Med. 2015;372:1019–1030. doi: 10.1056/NEJMoa1414905. - PubMed
-
- Saver JL, Goyal M, Bonafe A, Diener HC, Levy EI, Pereira VM, et al. SWIFT PRIME Investigators. Stent-retriever thrombectomy after intravenous t-PA vs. t-PA alone in stroke. N Engl J Med. 2015;372:2285–2295. doi: 10.1056/NEJMoa1415061. - PubMed
-
- Jovin TG, Chamorro A, Cobo E, de Miquel MA, Molina CA, Rovira A, et al. REVASCAT Trial Investigators. Thrombectomy within 8 hours after symptom onset in ischemic stroke. N Engl J Med. 2015;372:2296–2306. doi: 10.1056/NEJMoa1503780. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
