

Prespecified dose-response analysis for A Very Early Rehabilitation Trial (AVERT)
- PMID: 26888985
- PMCID: PMC4898313
- DOI: 10.1212/WNL.0000000000002459
Prespecified dose-response analysis for A Very Early Rehabilitation Trial (AVERT)
Erratum in
-
Correction: Prespecified dose-response analysis for A Very Early Rehabilitation Trial (AVERT).Neurology. 2017 Jul 4;89(1):107. doi: 10.1212/WNL.0000000000004107. Neurology. 2017. PMID: 28674163 No abstract available.
Abstract
Objective: Our prespecified dose-response analyses of A Very Early Rehabilitation Trial (AVERT) aim to provide practical guidance for clinicians on the timing, frequency, and amount of mobilization following acute stroke.
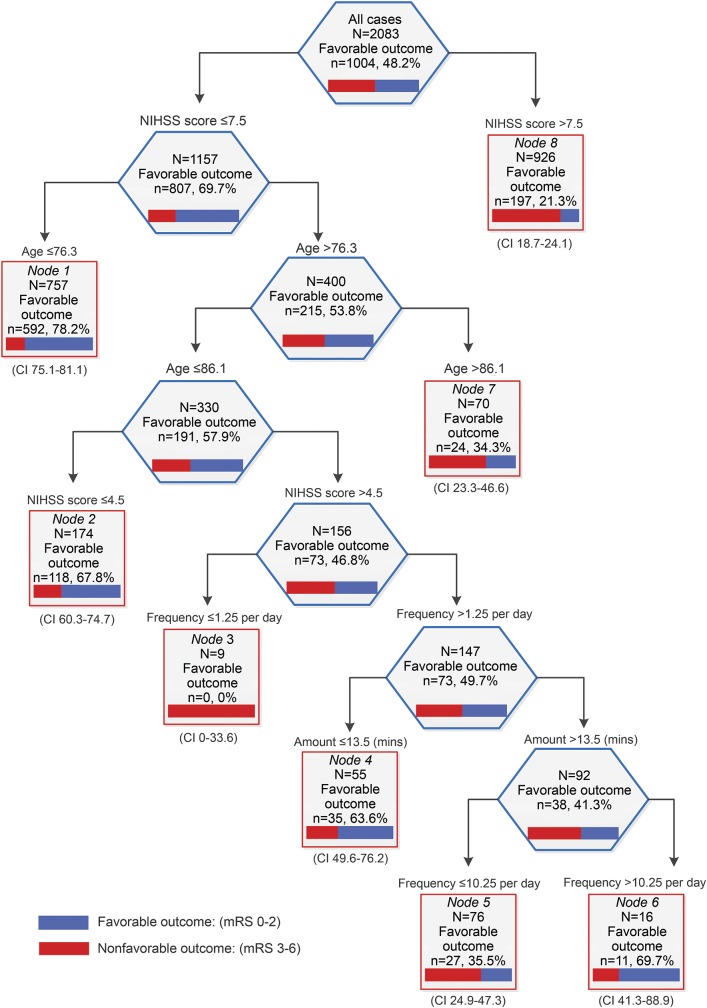
Methods: Eligible patients were aged ≥18 years, had confirmed first (or recurrent) stroke, and were admitted to a stroke unit within 24 hours of stroke onset. Patients were randomized to receive very early and frequent mobilization, commencing within 24 hours, or usual care. We used regression analyses and Classification and Regression Trees (CART) to investigate the effect of timing and dose of mobilization on efficacy and safety outcomes, irrespective of assigned treatment group.
Results: A total of 2,104 patients were enrolled, of whom 2,083 (99.0%) were followed up at 3 months. We found a consistent pattern of improved odds of favorable outcome in efficacy and safety outcomes with increased daily frequency of out-of-bed sessions (odds ratio [OR] 1.13, 95% confidence interval [CI] 1.09 to 1.18, p < 0.001), keeping time to first mobilization and mobilization amount constant. Increased amount (minutes per day) of mobilization reduced the odds of a good outcome (OR 0.94, 95% CI 0.91 to 0.97, p < 0.001). Session frequency was the most important variable in the CART analysis, after prognostic variables age and baseline stroke severity.
Conclusion: These data suggest that shorter, more frequent mobilization early after acute stroke is associated with greater odds of favorable outcome at 3 months when controlling for age and stroke severity.
Classification of evidence: This study provides Class III evidence that shorter, more frequent early mobilization improves the chance of regaining independence after stroke.
© 2016 American Academy of Neurology.
Figures
Comment in
-
Getting the right prescription for rehabilitation after stroke.Neurology. 2016 Jun 7;86(23):2120-1. doi: 10.1212/WNL.0000000000002653. Epub 2016 May 6. Neurology. 2016. PMID: 27164659 No abstract available.
References
-
- Bernhardt J, Langhorne P, Lindley R, et al. Efficacy and safety of very early mobilisation within 24 hours of stroke onset (AVERT): a randomised controlled trial. Lancet 2015;386:46–55. - PubMed
-
- van Wijk R, Cumming T, Churilov L, Donnan G, Bernhardt J. An early mobilization protocol successfully delivers more and earlier therapy to acute stroke patients: further results from phase II of AVERT. Neurorehabil Neural Repair 2012;26:20–26. - PubMed
-
- Indredavik B, Bakke RPT, Slordahl SA, Rokseth R, Haheim LL. Treatment in a combined acute and rehabilitation stroke unit: which aspects are most important? Stroke 1999;30:917–923. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials