

Neural Control of Walking in People with Parkinsonism
- PMID: 26889015
- PMCID: PMC4888974
- DOI: 10.1152/physiol.00034.2015
Neural Control of Walking in People with Parkinsonism
Abstract
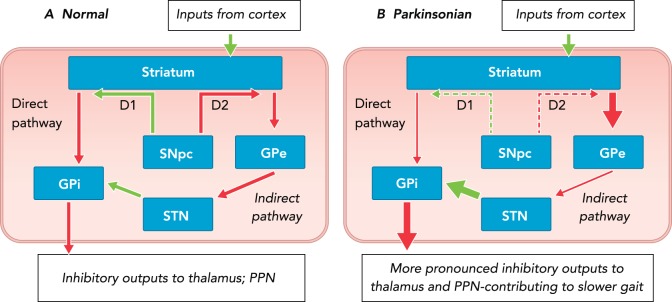
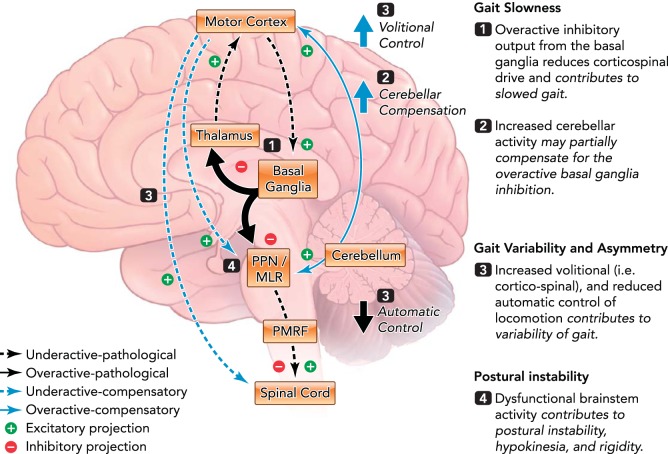
People with Parkinson's disease exhibit debilitating gait impairments, including gait slowness, increased step variability, and poor postural control. A widespread supraspinal locomotor network including the cortex, cerebellum, basal ganglia, and brain stem contributes to the control of human locomotion, and altered activity of these structures underlies gait dysfunction due to Parkinson's disease.
©2016 Int. Union Physiol. Sci./Am. Physiol. Soc.
Conflict of interest statement
F. B. Horak and OHSU have an equity/interest in APDM, a company that may have a commercial interest in the results of the study. This potential conflict of interest has been reviewed and managed by the Research & Development Committee at the Portland VA Medical Center and OHSU. No other authors declare any conflict of interest.
Figures

References
-
- Adkin AL, Bloem BR, Allum JH. Trunk sway measurements during stance and gait tasks in Parkinson's disease. Gait Posture 22: 240–249, 2005. - PubMed
-
- Albin RL, Young AB, Penney JB. The functional anatomy of basal ganglia disorders. Trends Neurosci 12: 366–375, 1989. - PubMed
-
- Baker R. Measuring Walking: A Handbook of Clinical Gait Analysis. Hoboken, NJ: Wiley, 2013.
-
- Baltadjieva R, Giladi N, Gruendlinger L, Peretz C, Hausdorff JM. Marked alterations in the gait timing and rhythmicity of patients with de novo Parkinson's disease. Eur J Neurosci 24: 1815–1820, 2006. - PubMed
-
- Blin O, Ferrandez AM, Pailhous J, Serratrice G. Dopa-sensitive and dopa-resistant gait parameters in Parkinson's disease. J Neurol Sci 103: 51–54, 1991. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical