

Long-Term Results of Stenting versus Endarterectomy for Carotid-Artery Stenosis
- PMID: 26890472
- PMCID: PMC4874663
- DOI: 10.1056/NEJMoa1505215
Long-Term Results of Stenting versus Endarterectomy for Carotid-Artery Stenosis
Abstract
Background: In the Carotid Revascularization Endarterectomy versus Stenting Trial, we found no significant difference between the stenting group and the endarterectomy group with respect to the primary composite end point of stroke, myocardial infarction, or death during the periprocedural period or any subsequent ipsilateral stroke during 4 years of follow-up. We now extend the results to 10 years.
Methods: Among patients with carotid-artery stenosis who had been randomly assigned to stenting or endarterectomy, we evaluated outcomes every 6 months for up to 10 years at 117 centers. In addition to assessing the primary composite end point, we assessed the primary end point for the long-term extension study, which was ipsilateral stroke after the periprocedural period.
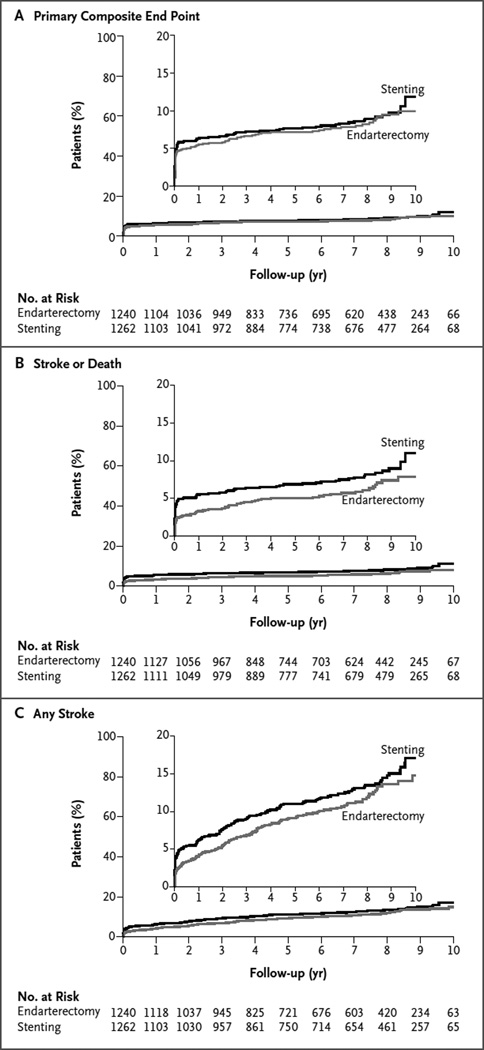
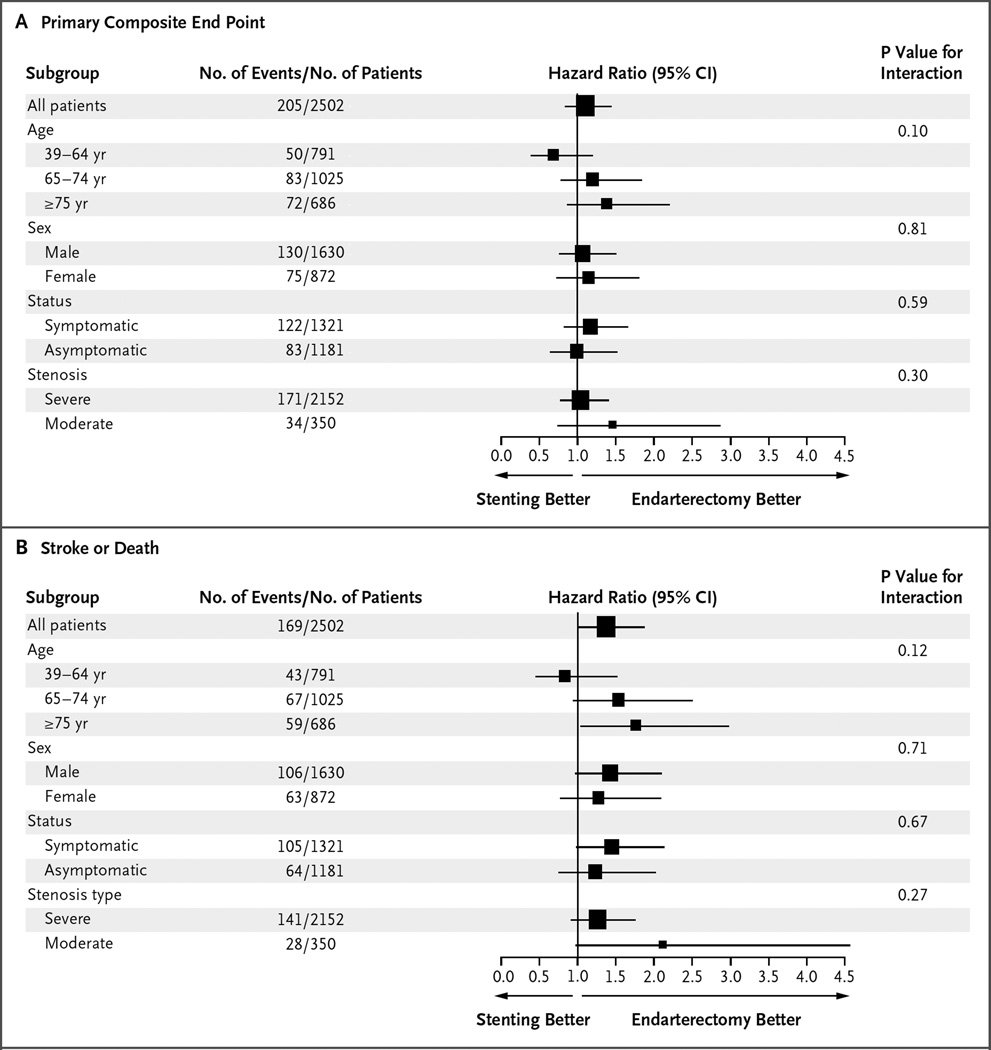
Results: Among 2502 patients, there was no significant difference in the rate of the primary composite end point between the stenting group (11.8%; 95% confidence interval [CI], 9.1 to 14.8) and the endarterectomy group (9.9%; 95% CI, 7.9 to 12.2) over 10 years of follow-up (hazard ratio, 1.10; 95% CI, 0.83 to 1.44). With respect to the primary long-term end point, postprocedural ipsilateral stroke over the 10-year follow-up occurred in 6.9% (95% CI, 4.4 to 9.7) of the patients in the stenting group and in 5.6% (95% CI, 3.7 to 7.6) of those in the endarterectomy group; the rates did not differ significantly between the groups (hazard ratio, 0.99; 95% CI, 0.64 to 1.52). No significant between-group differences with respect to either end point were detected when symptomatic patients and asymptomatic patients were analyzed separately.
Conclusions: Over 10 years of follow-up, we did not find a significant difference between patients who underwent stenting and those who underwent endarterectomy with respect to the risk of periprocedural stroke, myocardial infarction, or death and subsequent ipsilateral stroke. The rate of postprocedural ipsilateral stroke also did not differ between groups. (Funded by the National Institutes of Health and Abbott Vascular Solutions; CREST ClinicalTrials.gov number, NCT00004732.).
Figures
Comment in
-
Endarterectomy, Stenting, or Neither for Asymptomatic Carotid-Artery Stenosis.N Engl J Med. 2016 Mar 17;374(11):1087-8. doi: 10.1056/NEJMe1600123. Epub 2016 Feb 18. N Engl J Med. 2016. PMID: 26890473 No abstract available.
-
[Carotis stenosis: Stenting is eqivalent to endarteriectomy in the long term].Dtsch Med Wochenschr. 2016 May;141(10):678-9. doi: 10.1055/s-0042-103717. Epub 2016 May 13. Dtsch Med Wochenschr. 2016. PMID: 27176057 German. No abstract available.
-
Randomized Clinical Trial of Endovascular Stenting vs Endarterectomy for Treatment of Severe Carotid Stenosis.Neurosurgery. 2016 Aug;79(2):N20-2. doi: 10.1227/01.neu.0000489890.47483.49. Neurosurgery. 2016. PMID: 27428641 No abstract available.
-
Stenting versus Surgery for Carotid Stenosis.N Engl J Med. 2016 Aug 11;375(6):601-2. doi: 10.1056/NEJMc1605166. N Engl J Med. 2016. PMID: 27509115 No abstract available.
-
Stenting versus Surgery for Carotid Stenosis.N Engl J Med. 2016 Aug 11;375(6):602. doi: 10.1056/NEJMc1605166. N Engl J Med. 2016. PMID: 27509116 No abstract available.
-
Stenting versus Surgery for Carotid Stenosis.N Engl J Med. 2016 Aug 11;375(6):603. doi: 10.1056/NEJMc1605166. N Engl J Med. 2016. PMID: 27509118 No abstract available.
-
Stenting versus Surgery for Carotid Stenosis.N Engl J Med. 2016 Aug 11;375(6):604-5. doi: 10.1056/NEJMc1605166. N Engl J Med. 2016. PMID: 27517107 No abstract available.
References
-
- Office of the Chief Actuary (U.S.) Actuarial life table: period life table. Baltimore: Social Security Administration; 2011. https://www.ssa.gov/oact/STATS/table4c6.html.
-
- Hobson RW., II CREST (Carotid Revascularization Endarterectomy versus Stent Trial): background, design, and current status. Semin Vasc Surg. 2000;13:139–143. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical