

Restoration of Fornix Tear Reservoir in Conjunctivochalasis With Fornix Reconstruction
- PMID: 26890668
- PMCID: PMC4860082
- DOI: 10.1097/ICO.0000000000000784
Restoration of Fornix Tear Reservoir in Conjunctivochalasis With Fornix Reconstruction
Abstract
Purpose: To determine whether conjunctivochalasis (CCh) obliterates the fornix tear reservoir and to discern whether there is concomitant aqueous tear deficiency (ATD) dry eye.
Methods: Retrospective review of 18 eyes of 12 patients with CCh and ATD (CCh + ATD) and 18 eyes of 13 patients with CCh without ATD (CCh - ATD). Changes were compared before and after fornix reconstruction regarding symptoms, basal tear volumes, use of medications, conjunctival inflammation, and corneal staining.
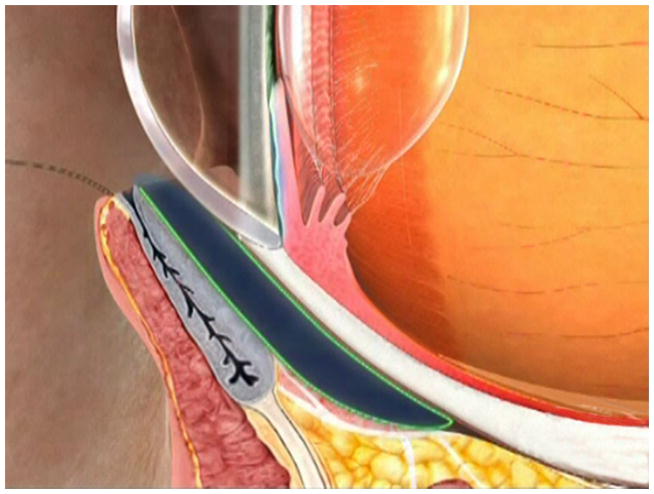
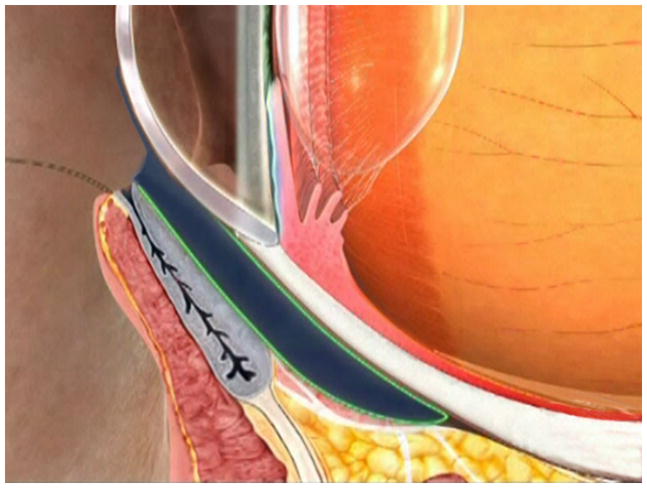
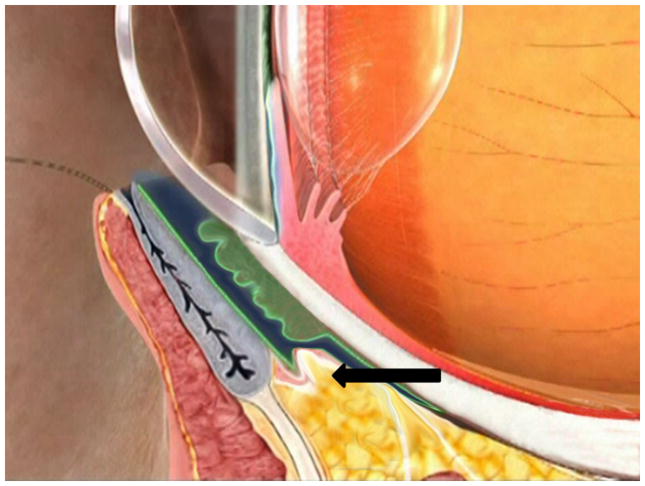
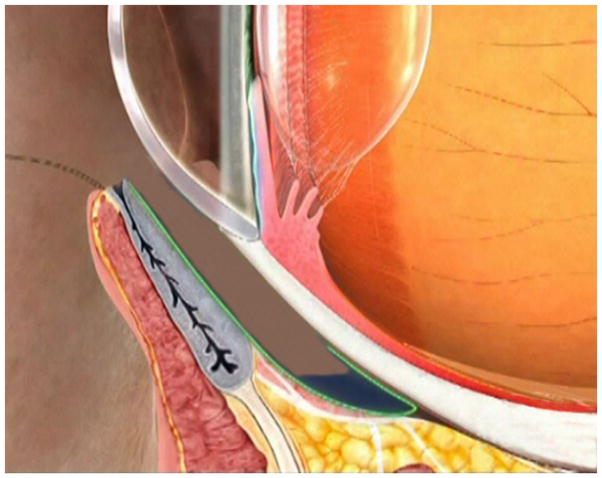
Results: Fornix reconstruction with conjunctival recession and amniotic membrane transplantation effectively restored the fornix tear reservoir as evidenced by a significant increase of the basal tear volume in both CCh - ATD and CCh + ATD groups. Multivariate regression analysis confirmed that such improvement was significantly correlated with symptomatic resolution (r = 1, P < 0.001), which was also accompanied by significant resolution of corneal staining, conjunctival inflammation, and reduction of topical medications. Intriguingly, the prior diagnosis of ATD was no longer existent in 10 of the 18 eyes (56%) with CCh + ATD suggesting that ATD could be secondary to obliteration of the fornix tear reservoir by CCh.
Conclusions: Obliteration of the fornix tear reservoir is a common pathogenic process regardless of whether CCh is associated with ATD dry eye. Restoration of the tear reservoir by fornix reconstruction with conjunctival recession and amniotic membrane transplantation results in significant resolution of symptoms and signs associated with ATD that is secondary to CCh and helps identify genuine ATD dry eye that is independent of CCh.
Figures
References
-
- Tseng SC, Tsubota K. Important concepts for treating ocular surface and tear disorders. Am J Ophthalmol. 1997;124(6):825–835. - PubMed
-
- Tseng SC. A practical treatment algorithm for managing ocular surface and tear disorders. Cornea. 2011;30(Suppl 1):S8–S14. - PubMed
-
- Mishima S, Gasset A, Klyce SD, et al. Determination of tear volume and tear flow. Invest Ophthalmol. 1966;5(3):264–276. - PubMed
-
- Meller D, Tseng SC. Conjunctivochalasis: literature review and possible pathophysiology. Surv Ophthalmol. 1998;43(3):225–232. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
