

Decompressive laparotomy for abdominal compartment syndrome
- PMID: 26891380
- PMCID: PMC5067589
- DOI: 10.1002/bjs.10097
Decompressive laparotomy for abdominal compartment syndrome
Abstract
Background: The effect of decompressive laparotomy on outcomes in patients with abdominal compartment syndrome has been poorly investigated. The aim of this prospective cohort study was to describe the effect of decompressive laparotomy for abdominal compartment syndrome on organ function and outcomes.
Methods: This was a prospective cohort study in adult patients who underwent decompressive laparotomy for abdominal compartment syndrome. The primary endpoints were 28-day and 1-year all-cause mortality. Changes in intra-abdominal pressure (IAP) and organ function, and laparotomy-related morbidity were secondary endpoints.
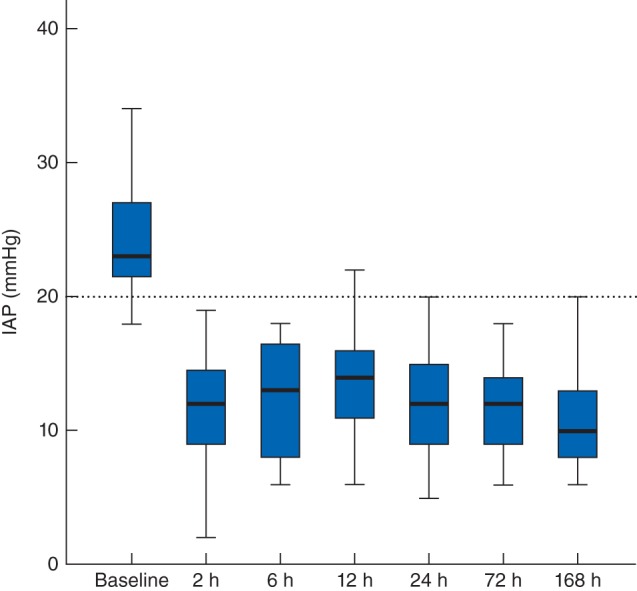
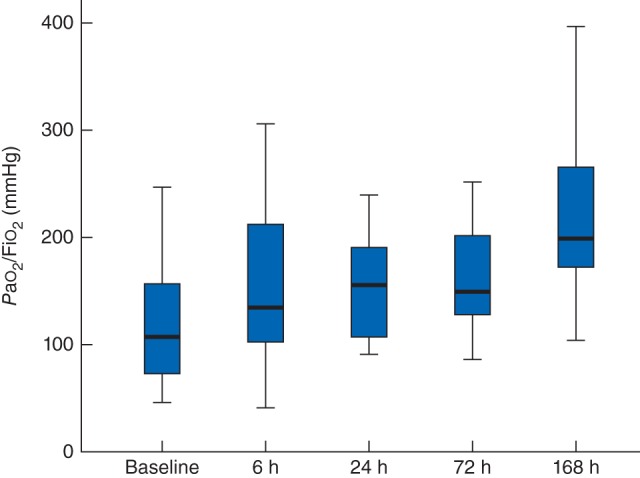
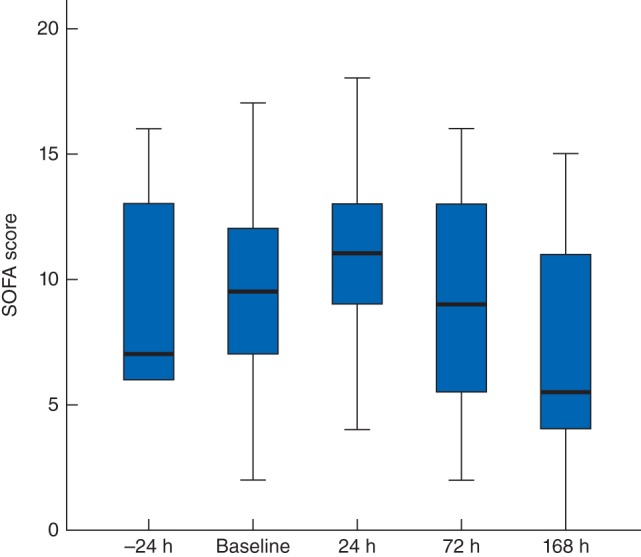
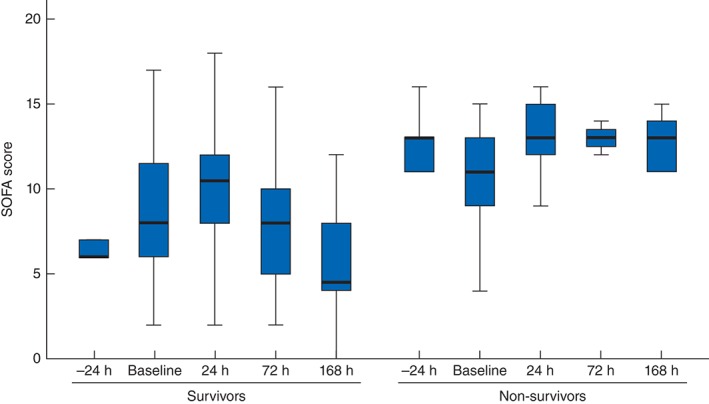
Results: Thirty-three patients were included in the study (20 men). Twenty-seven patients were surgical admissions treated for abdominal conditions. The median (i.q.r.) Acute Physiology And Chronic Health Evaluation (APACHE) II score was 26 (20-32). Median IAP was 23 (21-27) mmHg before decompressive laparotomy, decreasing to 12 (9-15), 13 (8-17), 12 (9-15) and 12 (9-14) mmHg after 2, 6, 24 and 72 h. Decompressive laparotomy significantly improved oxygenation and urinary output. Survivors showed improvement in organ function scores, but non-survivors did not. Fourteen complications related to the procedure developed in eight of the 33 patients. The abdomen could be closed primarily in 18 patients. The overall 28-day mortality rate was 36 per cent (12 of 33), which increased to 55 per cent (18 patients) at 1 year. Non-survivors were no different from survivors, except that they tended to be older and on mechanical ventilation.
Conclusion: Decompressive laparotomy reduced IAP and had an immediate effect on organ function. It should be considered in patients with abdominal compartment syndrome.
© 2016 The Authors. BJS published by John Wiley & Sons Ltd on behalf of BJS Society Ltd.
Figures
Comment in
-
Editor's Choice - Abdominal Compartment Syndrome After Surgery for Abdominal Aortic Aneurysm: A Nationwide Population Based Study.Eur J Vasc Endovasc Surg. 2016 Aug;52(2):158-65. doi: 10.1016/j.ejvs.2016.03.011. Epub 2016 Apr 20. Eur J Vasc Endovasc Surg. 2016. PMID: 27107488
References
-
- Schein M, Ivatury R. Intra‐abdominal hypertension and the abdominal compartment syndrome. Br J Surg 1998; 85: 1027–1028. - PubMed
-
- Balogh Z, McKinley BA, Cocanour CS, Kozar RA, Holcomb JB, Ware DN et al Secondary abdominal compartment syndrome is an elusive early complication of traumatic shock resuscitation. Am J Surg 2002; 184: 538–543. - PubMed
-
- Ertel W, Oberholzer A, Platz A, Stocker R, Trentz O. Incidence and clinical pattern of the abdominal compartment syndrome after ‘damage‐control’ laparotomy in 311 patients with severe abdominal and/or pelvic trauma. Crit Care Med 2000; 28: 1747–1753. - PubMed
-
- Ivatury RR, Porter JM, Simon RJ, Islam S, John R, Stahl WM. Intra‐abdominal hypertension after life‐threatening penetrating abdominal trauma: prophylaxis, incidence, and clinical relevance to gastric mucosal pH and abdominal compartment syndrome. J Trauma 1998; 44: 1016–1021. - PubMed
-
- Malbrain ML, Chiumello D, Pelosi P, Bihari D, Innes R, Ranieri VM et al Incidence and prognosis of intraabdominal hypertension in a mixed population of critically ill patients: a multiple‐center epidemiological study. Crit Care Med 2005; 33: 315–322. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
