

Plasma Levels of Endothelial Microparticles Bearing Monomeric C-reactive Protein are Increased in Peripheral Artery Disease
- PMID: 26891844
- PMCID: PMC4874871
- DOI: 10.1007/s12265-016-9678-0
Plasma Levels of Endothelial Microparticles Bearing Monomeric C-reactive Protein are Increased in Peripheral Artery Disease
Abstract
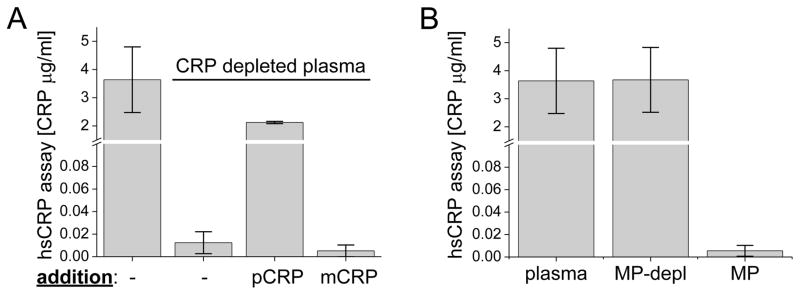
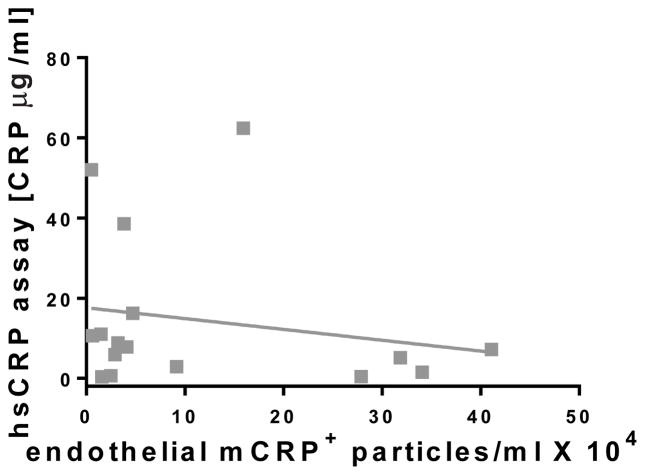
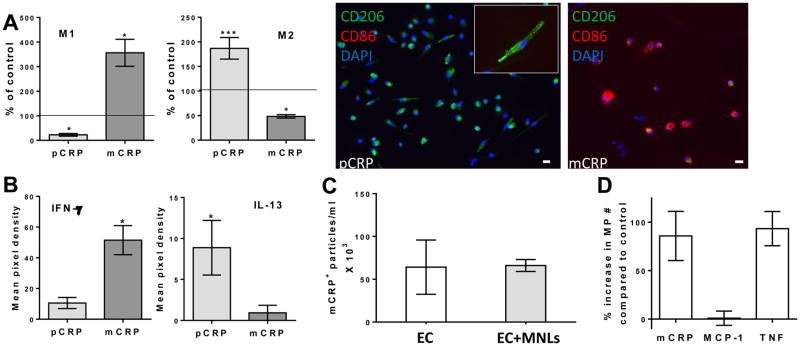
C-reactive protein (CRP) as an indicator of cardiovascular disease (CVD) has shown limited sensitivity. We demonstrate that two isoforms of CRP (pentameric, pCRP and monomeric, mCRP) present in soluble form or on microparticles (MPs) have different biological effects and are not all measured by clinical CRP assays. The high-sensitivity CRP assay (hsCRP) did not measure pCRP or mCRP on MPs, whereas flow cytometry did. MPs derived from endothelial cells, particularly those bearing mCRP, were elevated in peripheral artery disease (PAD) patients compared to controls. The numbers of mCRP(+) endothelial MPs did not correlate with hsCRP measurements of soluble pCRP, indicating their independent modulation. In controls, statins lowered mCRP(+) endothelial MPs. In a model of vascular inflammation, mCRP induced endothelial shedding of MPs and was proinflammatory, while pCRP was anti-inflammatory. mCRP on endothelial MPs may be both an unmeasured indicator of, and an amplifier of, vascular disease, and its detection might improve risk sensitivity.
Keywords: CRP; Inflammation; Microparticle; Monomeric CRP; Pentameric CRP; Peripheral artery disease; hsCRP.
Figures


Similar articles
-
A biofunctional review of C-reactive protein (CRP) as a mediator of inflammatory and immune responses: differentiating pentameric and modified CRP isoform effects.Front Immunol. 2023 Sep 15;14:1264383. doi: 10.3389/fimmu.2023.1264383. eCollection 2023. Front Immunol. 2023. PMID: 37781355 Free PMC article. Review.
-
Circulating microparticles generate and transport monomeric C-reactive protein in patients with myocardial infarction.Cardiovasc Res. 2012 Oct 1;96(1):64-72. doi: 10.1093/cvr/cvs237. Epub 2012 Jul 13. Cardiovasc Res. 2012. PMID: 22798388
-
The role of C-reactive protein in innate and acquired inflammation: new perspectives.Inflamm Cell Signal. 2016;3(2):e1409. Epub 2016 Sep 5. Inflamm Cell Signal. 2016. PMID: 27738646 Free PMC article.
-
Dissociation of pentameric to monomeric C-reactive protein on activated platelets localizes inflammation to atherosclerotic plaques.Circ Res. 2009 Jul 17;105(2):128-37. doi: 10.1161/CIRCRESAHA.108.190611. Epub 2009 Jun 11. Circ Res. 2009. PMID: 19520972
-
Dissociation of C-Reactive Protein Localizes and Amplifies Inflammation: Evidence for a Direct Biological Role of C-Reactive Protein and Its Conformational Changes.Front Immunol. 2018 Jun 12;9:1351. doi: 10.3389/fimmu.2018.01351. eCollection 2018. Front Immunol. 2018. PMID: 29946323 Free PMC article. Review.
Cited by
-
A biofunctional review of C-reactive protein (CRP) as a mediator of inflammatory and immune responses: differentiating pentameric and modified CRP isoform effects.Front Immunol. 2023 Sep 15;14:1264383. doi: 10.3389/fimmu.2023.1264383. eCollection 2023. Front Immunol. 2023. PMID: 37781355 Free PMC article. Review.
-
The Pathogenic Role of C-Reactive Protein in Diabetes-Linked Unstable Atherosclerosis.Int J Mol Sci. 2025 Jul 17;26(14):6855. doi: 10.3390/ijms26146855. Int J Mol Sci. 2025. PMID: 40725102 Free PMC article. Review.
-
Extracellular vesicles are associated with C-reactive protein in sepsis.Sci Rep. 2021 Mar 26;11(1):6996. doi: 10.1038/s41598-021-86489-4. Sci Rep. 2021. PMID: 33772103 Free PMC article.
-
A meta-analysis investigating the relationship between inflammation in autoimmune disease, elevated CRP, and the risk of dementia.Front Immunol. 2023 Jan 27;14:1087571. doi: 10.3389/fimmu.2023.1087571. eCollection 2023. Front Immunol. 2023. PMID: 36776896 Free PMC article. Review.
-
The monomeric C-reactive protein level is associated with the increase in carotid plaque number in patients with subclinical carotid atherosclerosis.Front Cardiovasc Med. 2022 Jul 22;9:968267. doi: 10.3389/fcvm.2022.968267. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 35935662 Free PMC article.
References
-
- Eisenhardt SU, Habersberger J, Murphy A, Chen YC, Woollard KJ, Bassler N, et al. Dissociation of pentameric to monomeric C-reactive protein on activated platelets localizes inflammation to atherosclerotic plaques. Circulation research. 2009;105(2):128–137. doi: 10.1161/CIRCRESAHA.108.190611. - DOI - PubMed
-
- Hirschfield GM, Gallimore JR, Kahan MC, Hutchinson WL, Sabin CA, Benson GM, et al. Transgenic human C-reactive protein is not proatherogenic in apolipoprotein E-deficient mice. Proceedings of the National Academy of Sciences of the United States of America. 2005;102(23):8309–8314. doi: 10.1073/pnas.0503202102. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
