

Gait analysis before and after corrective osteotomy in patients with knee osteoarthritis and a valgus deformity
- PMID: 26891964
- PMCID: PMC5570791
- DOI: 10.1007/s00167-016-4045-x
Gait analysis before and after corrective osteotomy in patients with knee osteoarthritis and a valgus deformity
Abstract
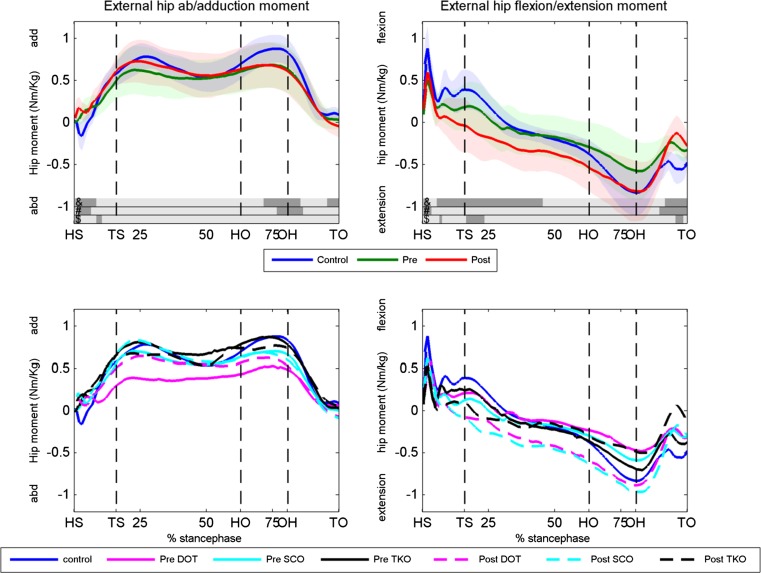
Purpose: In this prospective study, the changes in kinetics and kinematics of gait and clinical outcomes after a varus osteotomy (tibial, femoral or double osteotomy) in patients with osteoarthritis (OA) of the knee and a valgus leg alignment were analysed and compared to healthy subjects.
Methods: Twelve patients and ten healthy controls were included. Both kinetics and kinematics of gait and clinical and radiographic outcomes were evaluated.
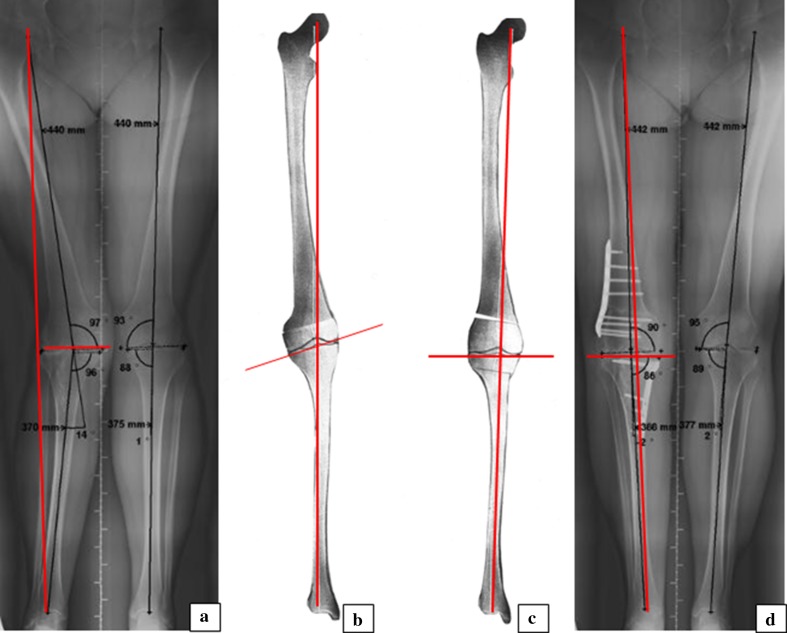
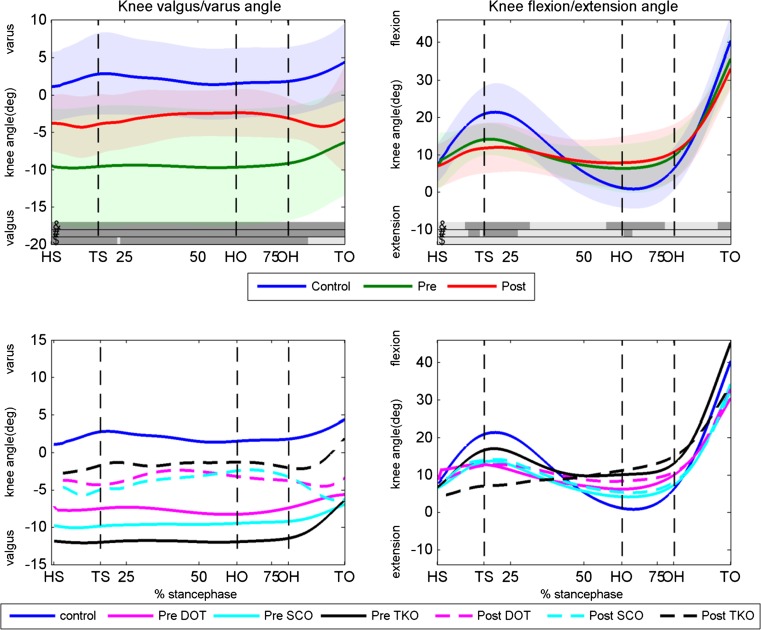
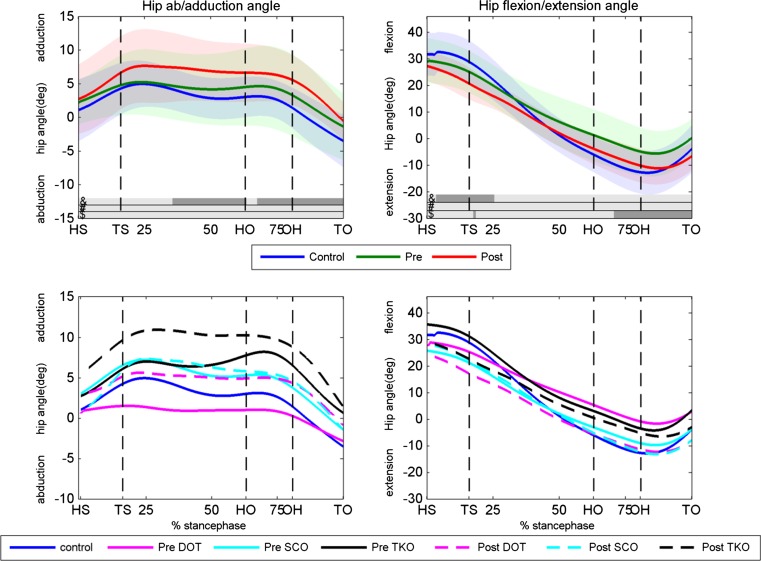
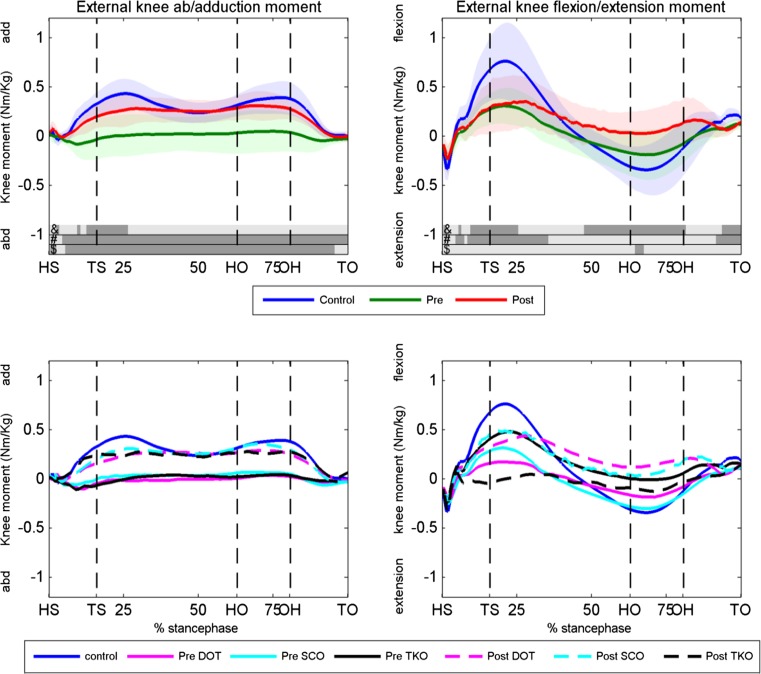
Results: The knee adduction moment increased significantly postoperatively (p < 0.05) and almost similar to the control group. Patients showed less knee and hip flexion/extension motion and moment during gait pre- and postoperatively compared to the controls. A significant improvement was found in WOMAC [80.8 (SD 16.1), p = 0.000], KOS [74.9 (SD 14.7), p = 0.018], OKS [21.2 (SD 7.5), p = 0.000] and VAS-pain [32.9 (SD 20.9), p = 0.003] in all patients irrespective of the osteotomy technique used. The radiographic measurements showed a mean hip knee ankle (HKA) angle correction of 10.4° (95 % CI 6.4°-14.4°).
Conclusion: In patients with knee OA combined with a valgus leg alignment, the varus-producing osteotomy is a successful treatment. Postoperatively, the patients showed kinetics and kinematics of gait similar as that of a healthy control group. A significant increase in the knee adduction moment during stance phase was found, which was related to the degree of correction. The HKA angle towards zero degrees caused a medial shift in the dynamic knee loading. The medial shift will optimally restore cartilage loading forces and knee ligament balance and reduces progression of OA or the risk of OA. A significant improvement in all clinical outcomes was also found.
Level of evidence: III.
Keywords: Closed wedge medial high tibial osteotomy; Double osteotomy; Gait analysis; Supracondylar femoral osteotomy; Valgus alignment.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
References
-
- Aglietti P, Menchetti PP. Distal femoral varus osteotomy in the valgus osteoarthritic knee. Am J Knee Surg. 2000;13(2):89–95. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
