

Targeted antibiotic delivery using low temperature-sensitive liposomes and magnetic resonance-guided high-intensity focused ultrasound hyperthermia
- PMID: 26892114
- PMCID: PMC6029942
- DOI: 10.3109/02656736.2015.1134818
Targeted antibiotic delivery using low temperature-sensitive liposomes and magnetic resonance-guided high-intensity focused ultrasound hyperthermia
Abstract
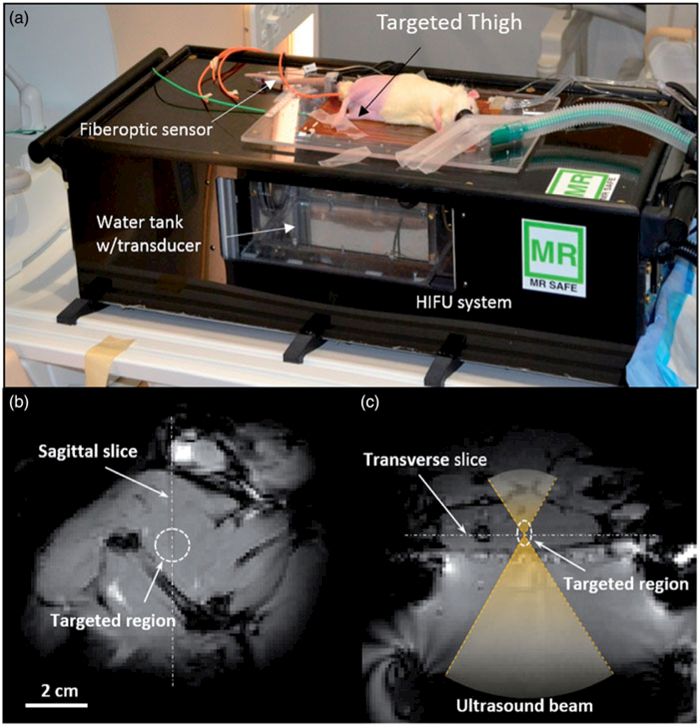
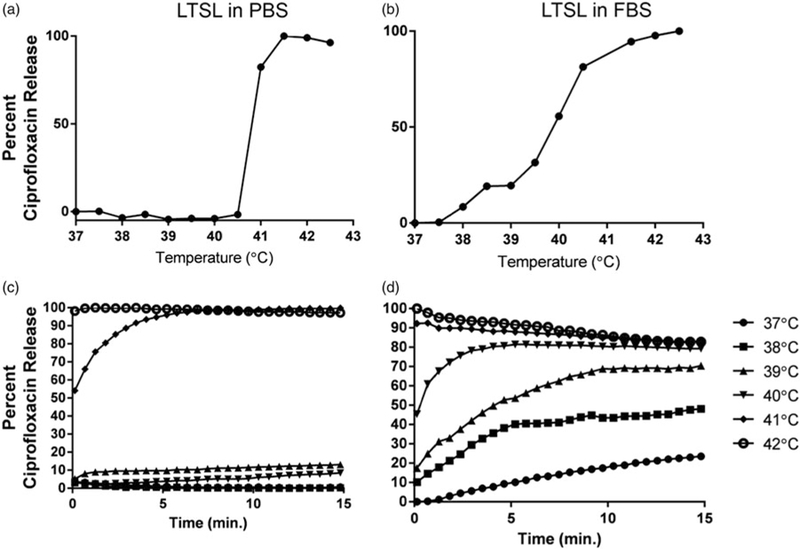
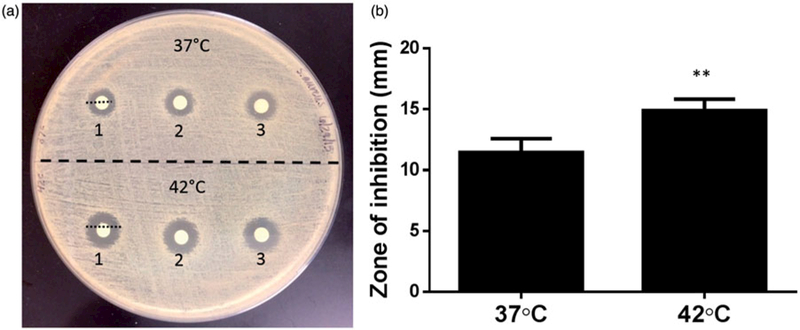
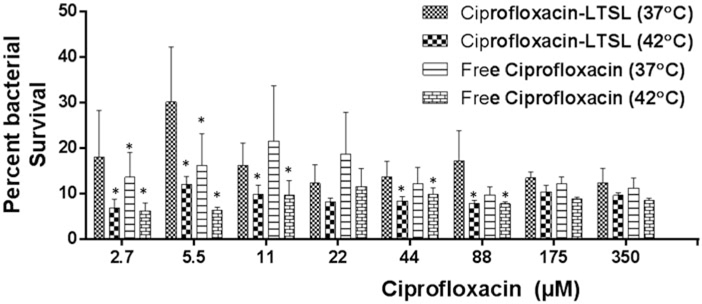
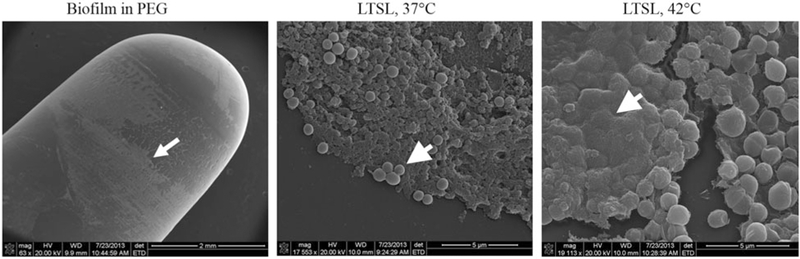
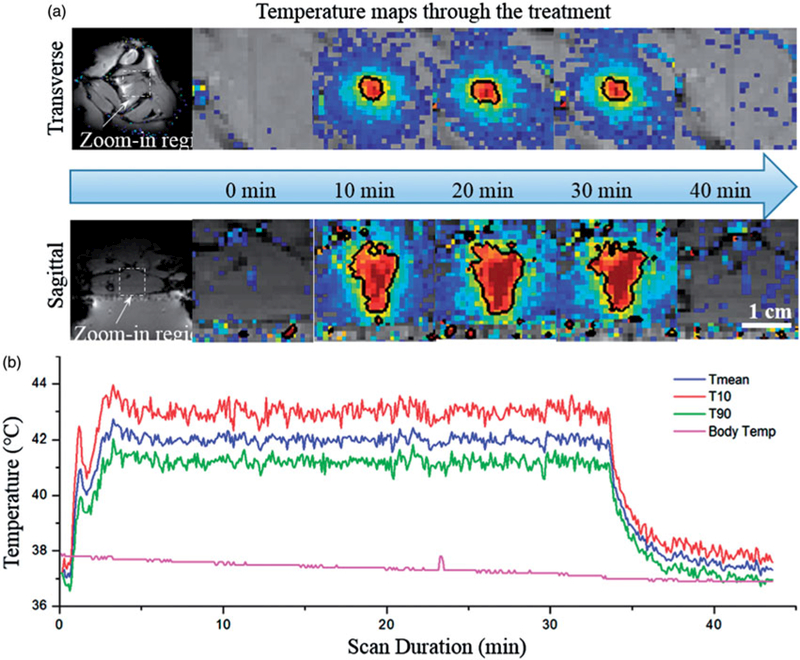
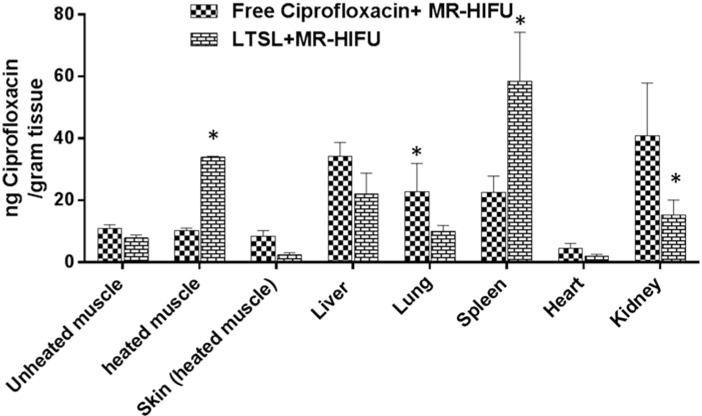
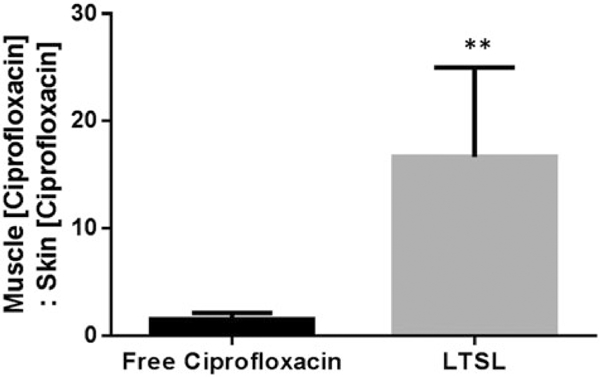
Chronic non-healing wound infections require long duration antibiotic therapy, and are associated with significant morbidity and health-care costs. Novel approaches for efficient, readily-translatable targeted and localised antimicrobial delivery are needed. The objectives of this study were to 1) develop low temperature-sensitive liposomes (LTSLs) containing an antimicrobial agent (ciprofloxacin) for induced release at mild hyperthermia (∼42 °C), 2) characterise in vitro ciprofloxacin release, and efficacy against Staphylococcus aureus plankton and biofilms, and 3) determine the feasibility of localised ciprofloxacin delivery in combination with MR-HIFU hyperthermia in a rat model. LTSLs were loaded actively with ciprofloxacin and their efficacy was determined using a disc diffusion method, MBEC biofilm device, and scanning electron microscopy (SEM). Ciprofloxacin release from LTSLs was assessed in a physiological buffer by fluorescence spectroscopy, and in vivo in a rat model using MR-HIFU. Results indicated that < 5% ciprofloxacin was released from the LTSL at body temperature (37 °C), while >95% was released at 42 °C. Precise hyperthermia exposures in the thigh of rats using MR-HIFU during intravenous (i.v.) administration of the LTSLs resulted in a four fold greater local concentration of ciprofloxacin compared to controls (free ciprofloxacin + MR-HIFU or LTSL alone). The biodistribution of ciprofloxacin in unheated tissues was fairly similar between treatment groups. Triggered release at 42 °C from LTSL achieved significantly greater S. aureus killing and induced membrane deformation and changes in biofilm matrix compared to free ciprofloxacin or LTSL at 37 °C. This technique has potential as a method to deliver high concentration antimicrobials to chronic wounds.
Keywords: Chronic wound; MR-HIFU; image guided therapy; low temperature-sensitive liposomes (LTSL); triggered antibiotic release.
Figures
References
-
- Siddiqui AR, Bernstein JM. Chronic wound infection: Facts and controversies. Clin Dermatol 2010;28:519–26. - PubMed
-
- Sibbald RG, Woo K, Ayello EA. Increased bacterial burden and infection: The story of NERDS and STONES. Adv Skin Wound Care 2006;19:447–61; quiz 61–3. - PubMed
-
- Lipsky BA, Hoey C. Topical antimicrobial therapy for treating chronic wounds. Clin Infect Dis 2009;49:1541–9. - PubMed
-
- Marriott R, Rubayi S. Successful truncated osteomyelitis treatment for chronic osteomyelitis secondary to pressure ulcers in spinal cord injury patients. Ann Plast Surg 2008;61:425–9. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical