

Diagnostic Strategies for the Evaluation of Chest Pain: Clinical Implications From SCOT-HEART and PROMISE
- PMID: 26892420
- PMCID: PMC4771619
- DOI: 10.1016/j.jacc.2015.11.055
Diagnostic Strategies for the Evaluation of Chest Pain: Clinical Implications From SCOT-HEART and PROMISE
Abstract
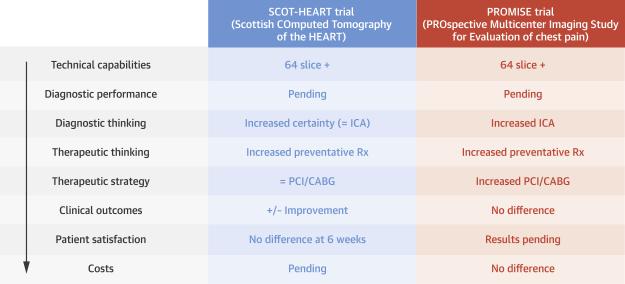
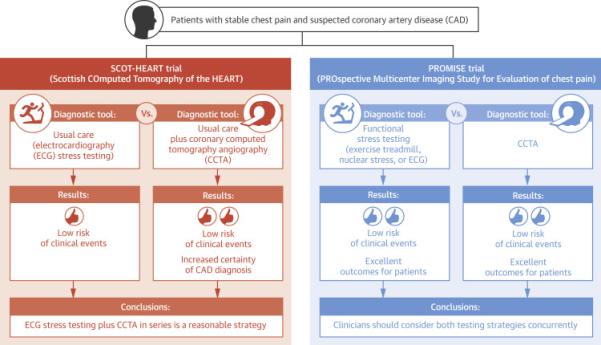
SCOT-HEART (Scottish COmputed Tomography of the HEART) and PROMISE (PROspective Multicenter Imaging Study for Evaluation of chest pain) represent the 2 largest and most comprehensive cardiovascular imaging outcome trials in patients with stable chest pain and provide significant insights into patient diagnosis, management, and outcomes. These trials are particularly timely, given the well-recognized knowledge gaps and widespread use of noninvasive imaging. The overall goal of this review is to distill the data generated from these 2 pivotal trials to better inform the practicing clinician in the selection of noninvasive testing for stable chest pain. Similarities and differences between SCOT-HEART and PROMISE are highlighted, and clinical and practical implications are discussed. Both trials show that coronary computed tomography angiography should have a greater role in the diagnostic pathway of patients with stable chest pain.
Keywords: angina pectoris; coronary artery disease; noninvasive cardiac imaging; patient selection.
Copyright © 2016 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Mozaffarian D, Benjamin EJ, Go AS, et al. American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics--2015 update: a report from the American Heart Association. Circulation. 2015;131:e29–322. - PubMed
-
- Daly CA, Clemens F, Sendon JLL, et al. The clinical characteristics and investigations planned in patients with stable angina presenting to cardiologists in Europe: from the Euro Heart Survey of Stable Angina. Eur Heart J. 2005;26:996–1010. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
