

The protective effect of trimetazidine on myocardial ischemia/reperfusion injury through activating AMPK and ERK signaling pathway
- PMID: 26892523
- PMCID: PMC4967934
- DOI: 10.1016/j.metabol.2015.10.022
The protective effect of trimetazidine on myocardial ischemia/reperfusion injury through activating AMPK and ERK signaling pathway
Abstract
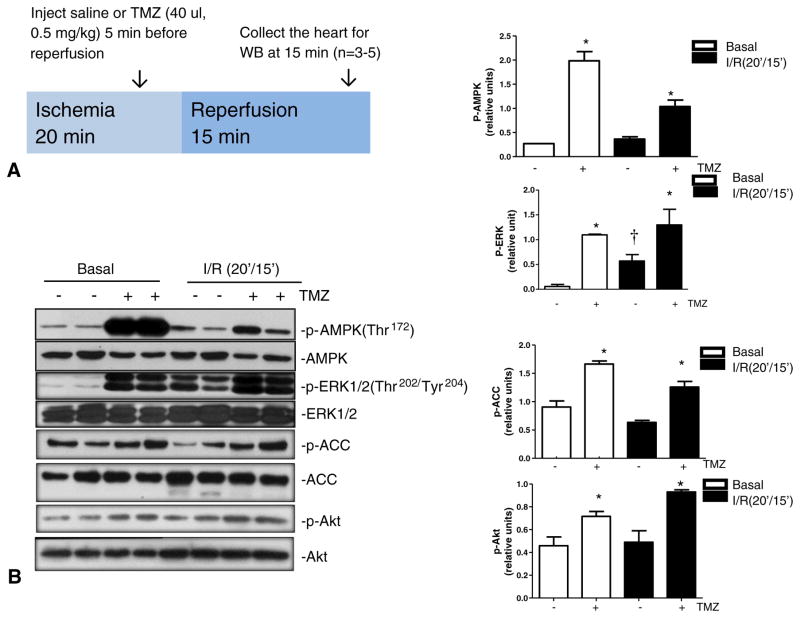
Introduction: Trimetazidine (TMZ) is an anti-anginal drug that has been widely used in Europe and Asia. The TMZ can optimize energy metabolism via inhibition of long-chain 3-ketoacyl CoA thiolase (3-KAT) in the heart, with subsequent decrease in fatty acid oxidation and stimulation of glucose oxidation. However, the mechanism by which TMZ aids in cardioprotection against ischemic injury has not been characterized. AMP-activated protein kinase (AMPK) is an energy sensor that controls ATP supply from substrate metabolism and protects heart from energy stress. TMZ changes the cardiac AMP/ATP ratio by modulating fatty acid oxidation, thereby triggering AMPK signaling cascade that contributes to the protection of the heart from ischemia/reperfusion (I/R) injury.
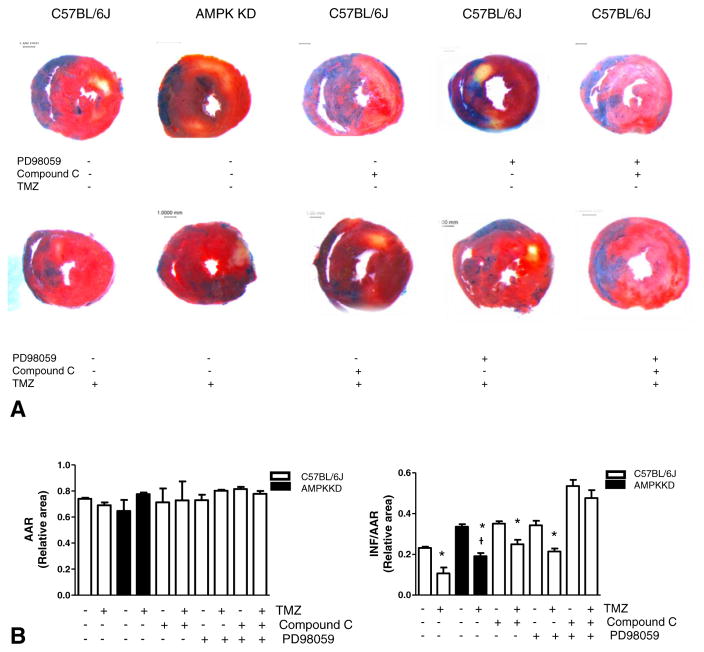
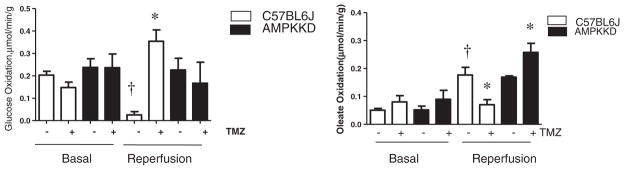
Methods: The mouse model of in vivo regional ischemia and reperfusion by the ligation of the left anterior descending coronary artery (LAD) was used for determination of myocardial infarction. The infarct size was compared between C57BL/6J WT mice and AMPK kinase dead (KD) transgenic mice with or without TMZ treatment. The ex vivo working heart perfusion system was used to monitor the effect of TMZ on glucose oxidation and fatty acid oxidation in the heart.
Results: TMZ treatment significantly stimulates cardiac AMPK and extracellular signal-regulated kinase (ERK) signaling pathways (p<0.05 vs. vehicle group). The administration of TMZ reduces myocardial infarction size in WT C57BL/6J hearts, the reduction of myocardial infarction size by TMZ in AMPK KD hearts was significantly impaired versus WT hearts (p<0.05). Intriguingly, the administration of ERK inhibitor, PD98059, to AMPK KD mice abolished the cardioprotection of TMZ against I/R injury. The ex vivo working heart perfusion data demonstrated that TMZ treatment significantly activates AMPK signaling and modulating the substrate metabolism by shifting fatty acid oxidation to glucose oxidation during reperfusion, leading to reduction of oxidative stress in the I/R hearts. Therefore, both AMPK and ERK signaling pathways mediate the cardioprotection of TMZ against ischemic injury. The metabolic benefits of TMZ for angina patients could be due to the activation of energy sensor AMPK in the heart by TMZ administration.
Keywords: AMPK signaling; Cardioprotection; Ischemia/reperfusion; MAPK signaling; Trimetazidine.
Copyright © 2015. Published by Elsevier Inc.
Conflict of interest statement
None.
Figures
References
-
- Murray CJ, Vos T, Lozano R, Naghavi M, Flaxman AD, Michaud C, et al. Disability-adjusted life years (DALYs) for 291 diseases and injuries in 21 regions, 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380:2197–223. - PubMed
-
- Go AS, Mozaffarian D, Roger VL, Benjamin EJ, Berry JD, Blaha MJ, et al. Executive summary: heart disease and stroke statistics —2014 update: a report from the American Heart Association. Circulation. 2014;129:399–410. - PubMed
-
- Worner F, Cequier A, Bardaji A, Bodi V, et al. Grupo de Trabajo de la Sociedad Espanola de Cardiologia para la guia de practica clinica sobre el sindrome coronario agudo con elevacion del segmento ST. Comments on the ESC guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation. Rev Esp Cardiol. 2013;66:5–11. Coordinadores. - PubMed
-
- Stanley WC, Marzilli M. Metabolic therapy in the treatment of ischaemic heart disease: the pharmacology of trimetazidine. Fundam Clin Pharmacol. 2003;17:133–45. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
