

Hereditary melanoma: Update on syndromes and management: Genetics of familial atypical multiple mole melanoma syndrome
- PMID: 26892650
- PMCID: PMC4761105
- DOI: 10.1016/j.jaad.2015.08.038
Hereditary melanoma: Update on syndromes and management: Genetics of familial atypical multiple mole melanoma syndrome
Abstract
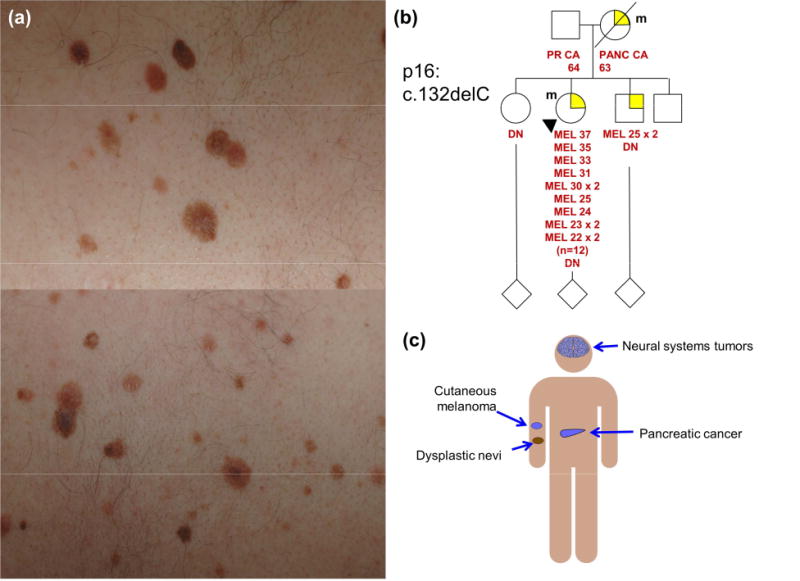
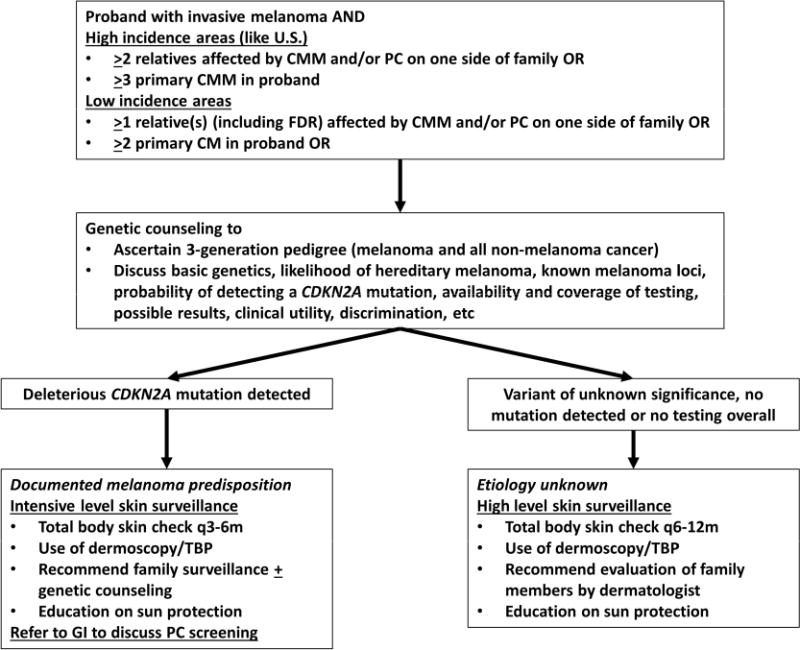
Malignant melanoma is considered the most lethal skin cancer if it is not detected and treated during its early stages. About 10% of melanoma patients report a family history of melanoma; however, individuals with features of true hereditary melanoma (ie, unilateral lineage, multigenerational, multiple primary lesions, and early onset of disease) are in fact quite rare. Although many new loci have been implicated in hereditary melanoma, CDKN2A mutations remain the most common. Familial melanoma in the presence of multiple atypical nevi should raise suspicion for a germline CDKN2A mutation. These patients have a high risk of developing multiple primary melanomas and internal organ malignancies, especially pancreatic cancer; therefore, a multidisciplinary approach is necessary in many cases. The value of dermoscopic examination and total body photography performed at regular intervals has been suggested by a number of studies, and should therefore be considered for these patients and their first-degree relatives. In addition, genetic counseling with the possibility of testing can be a valuable adjunct for familial melanoma patients. This must be performed with care, however, and only by qualified individuals trained in cancer risk analysis.
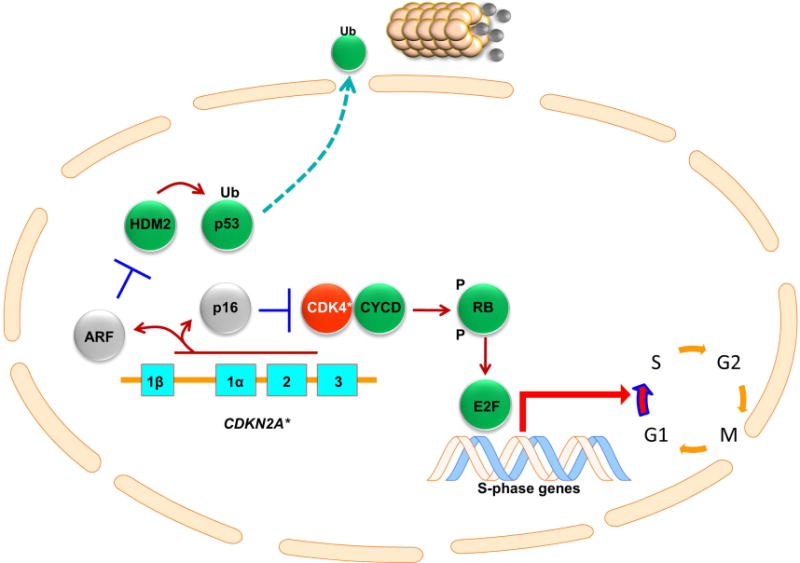
Keywords: CDK4; CDKN2A; FAMMM; familial melanoma syndromes; melanoma genetics; mixed cancer syndromes.
Copyright © 2015 American Academy of Dermatology, Inc. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
The absence of multiple atypical nevi in germline CDKN2A mutations: Comment on "Hereditary melanoma: Update on syndromes and management: Genetics of familial atypical multiple mole melanoma syndrome".J Am Acad Dermatol. 2016 Oct;75(4):e157. doi: 10.1016/j.jaad.2016.04.069. J Am Acad Dermatol. 2016. PMID: 27646763 No abstract available.
References
-
- Bray F, Jemal A, Grey N, Ferlay J, Forman D. Global cancer transitions according to the Human Development Index (2008–2030): a population-based study. Lancet Oncol. 2012;13(8):790–801. - PubMed
-
- Goldstein AM, Tucker MA. Genetic epidemiology of cutaneous melanoma: a global perspective. Arch Dermatol. 2001;137(11):1493–1496. - PubMed
-
- Goldstein AM, Chan M, Harland M, Gillanders EM, Hayward NK, Avril MF, Azizi E, Bianchi-Scarra G, Bishop DT, Bressac-de Paillerets B, Bruno W, Calista D, Cannon Albright LA, Demenais F, Elder DE, Ghiorzo P, Gruis NA, Hansson J, Hogg D, Holland EA, Kanetsky PA, Kefford RF, Landi MT, Lang J, Leachman SA, Mackie RM, Magnusson V, Mann GJ, Niendorf K, Newton Bishop J, Palmer JM, Puig S, Puig-Butille JA, de Snoo FA, Stark M, Tsao H, Tucker MA, Whitaker L, Yakobson E, Melanoma Genetics C High-risk melanoma susceptibility genes and pancreatic cancer, neural system tumors, and uveal melanoma across GenoMEL. Cancer Res. 2006;66(20):9818–9828. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
