

Genetic variation frequencies in Wilms' tumor: A meta-analysis and systematic review
- PMID: 26892980
- PMCID: PMC4970837
- DOI: 10.1111/cas.12910
Genetic variation frequencies in Wilms' tumor: A meta-analysis and systematic review
Abstract
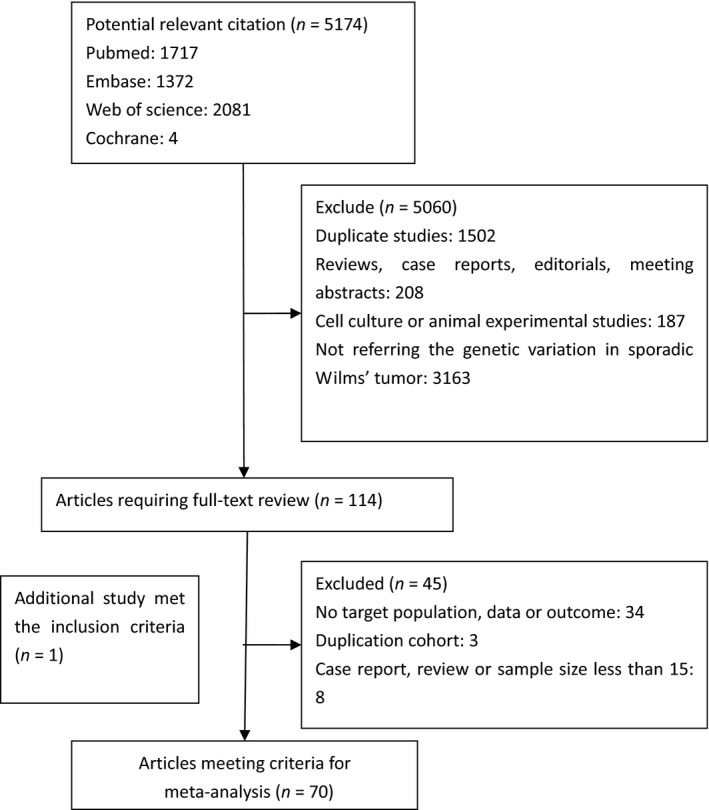
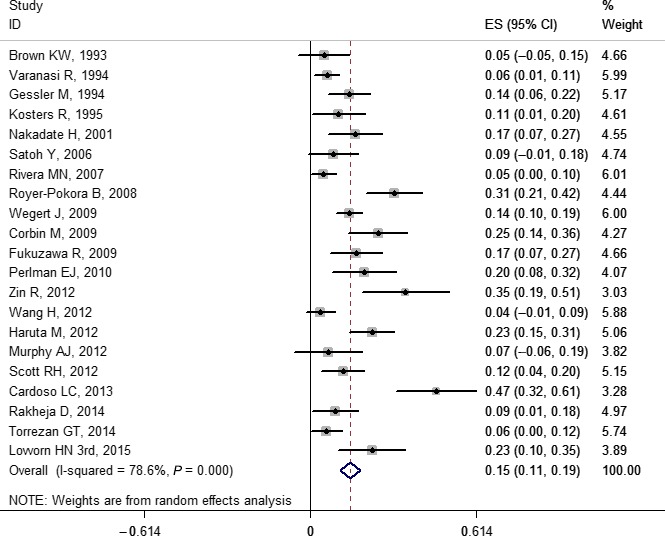
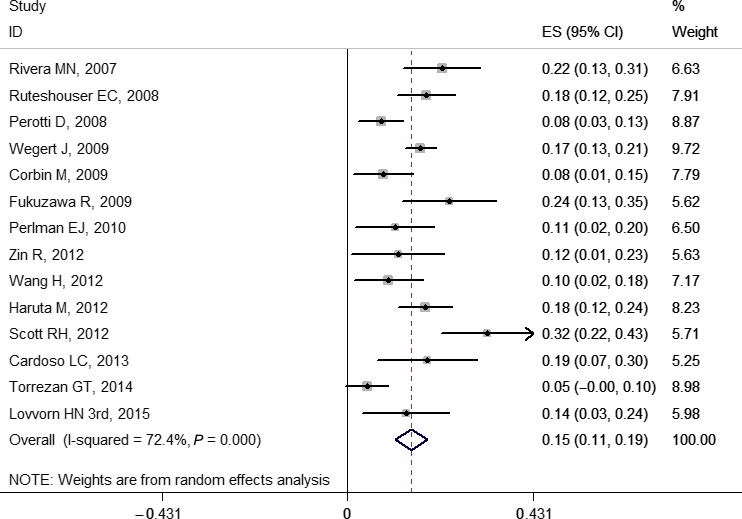
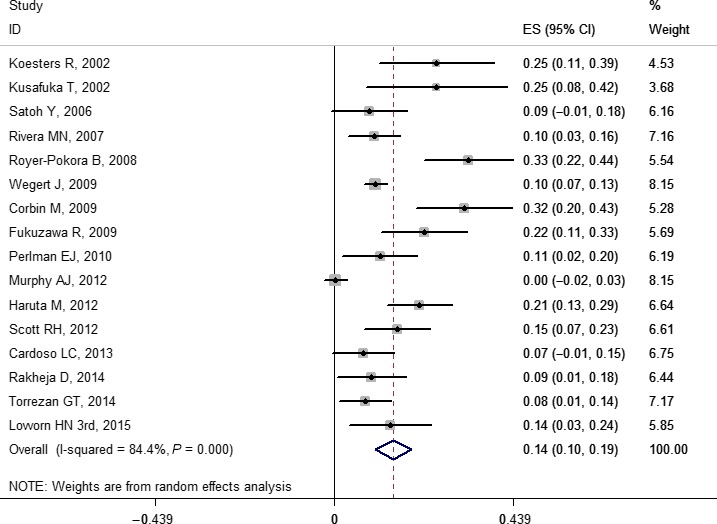
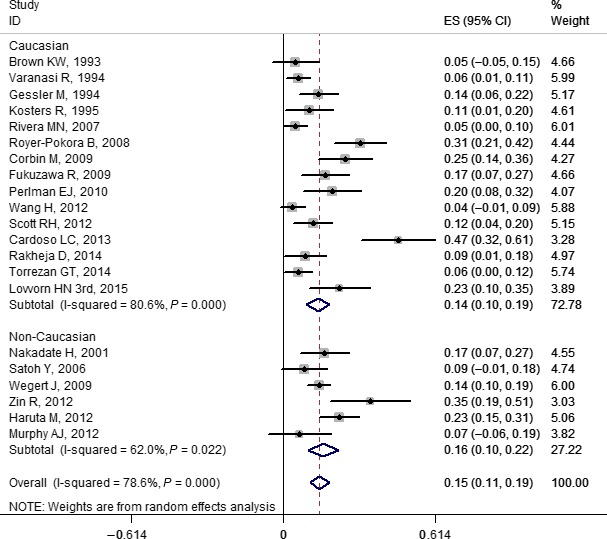
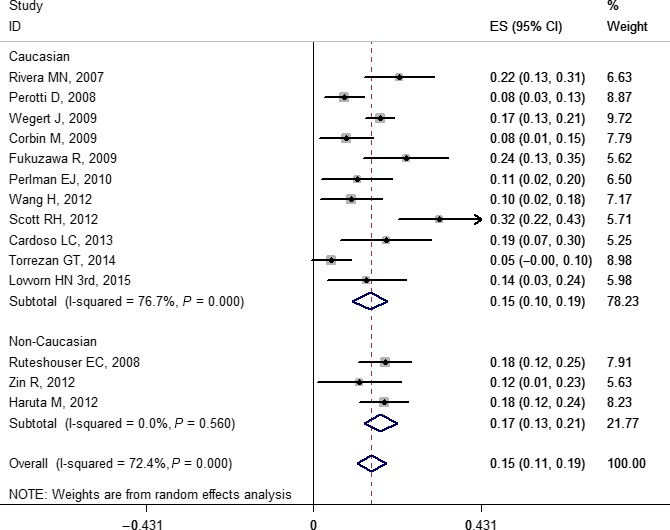
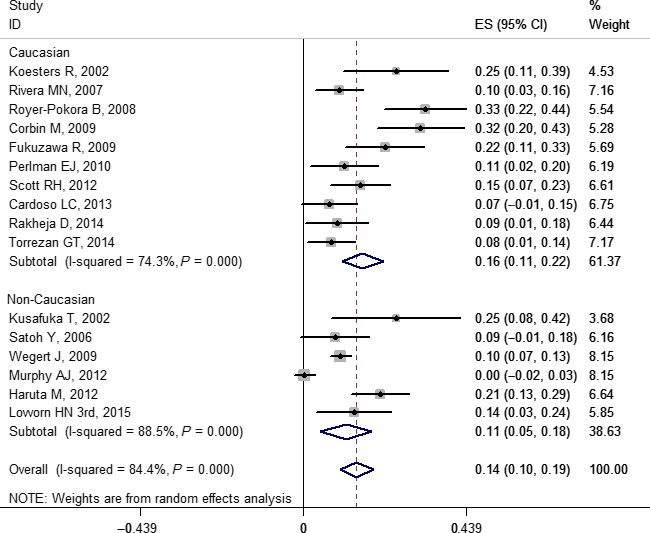
Over the last few decades, numerous biomarkers in Wilms' tumor have been confirmed and shown variations in prevalence. Most of these studies were based on small sample sizes. We carried out a meta-analysis of the research published from 1992 to 2015 to obtain more precise and comprehensive outcomes for genetic tests. In the present study, 70 out of 5175 published reports were eligible for the meta-analysis, which was carried out using Stata 12.0 software. Pooled prevalence for gene mutations WT1, WTX, CTNNB1, TP53, MYCN, DROSHA, and DGCR8 was 0.141 (0.104, 0.178), 0.147 (0.110, 0.184), 0.140 (0.100, 0.190), 0.410 (0.214, 0.605), 0.071 (0.041, 0.100), 0.082 (0.048, 0.116), and 0.036 (0.026, 0.046), respectively. Pooled prevalence of loss of heterozygosity at 1p, 11p, 11q, 16q, and 22q was 0.109 (0.084, 0.133), 0.334 (0.295, 0.373), 0.199 (0.146, 0.252), 0.151 (0.129, 0.172), and 0.148 (0.108, 0.189), respectively. Pooled prevalence of 1q and chromosome 12 gain was 0.218 (0.161, 0.275) and 0.273 (0.195, 0.350), respectively. The limited prevalence of currently known genetic alterations in Wilms' tumors indicates that significant drivers of initiation and progression remain to be discovered. Subgroup analyses indicated that ethnicity may be one of the sources of heterogeneity. However, in meta-regression analyses, no study-level characteristics of indicators were found to be significant. In addition, the findings of our sensitivity analysis and possible publication bias remind us to interpret results with caution.
Keywords: Children; Wilms' tumor; genetic variations; meta-analysis; prevalence.
© 2016 The Authors. Cancer Science published by John Wiley & Sons Australia, Ltd on behalf of Japanese Cancer Association.
Figures
References
-
- Breslow NE, Olson J, Moksness J, Beckwith JB, Grundy P. Familial Wilms' tumor: a descriptive study. Med Pediatr Oncol 1996; 27: 398–403. - PubMed
-
- Mcdonald JM, Douglass EC, Fisher R et al Linkage of familial Wilms' tumor predisposition to chromosome 19 and a two‐locus model for the etiology of familial tumors. Cancer Res 1998; 58: 1387–90. - PubMed
-
- Rahman N, Arbour L, Tonin P et al Evidence for a familial Wilms' tumour gene (FWT1) on chromosome 17q12‐q21. Nat Genet 1996; 13: 461–3. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
