

Incremental impact upon malaria transmission of supplementing pyrethroid-impregnated long-lasting insecticidal nets with indoor residual spraying using pyrethroids or the organophosphate, pirimiphos methyl
- PMID: 26893012
- PMCID: PMC4758014
- DOI: 10.1186/s12936-016-1143-7
Incremental impact upon malaria transmission of supplementing pyrethroid-impregnated long-lasting insecticidal nets with indoor residual spraying using pyrethroids or the organophosphate, pirimiphos methyl
Abstract
Background: Long-lasting, insecticidal nets (LLINs) and indoor residual spraying (IRS) are the most widely accepted and applied malaria vector control methods. However, evidence that incremental impact is achieved when they are combined remains limited and inconsistent.
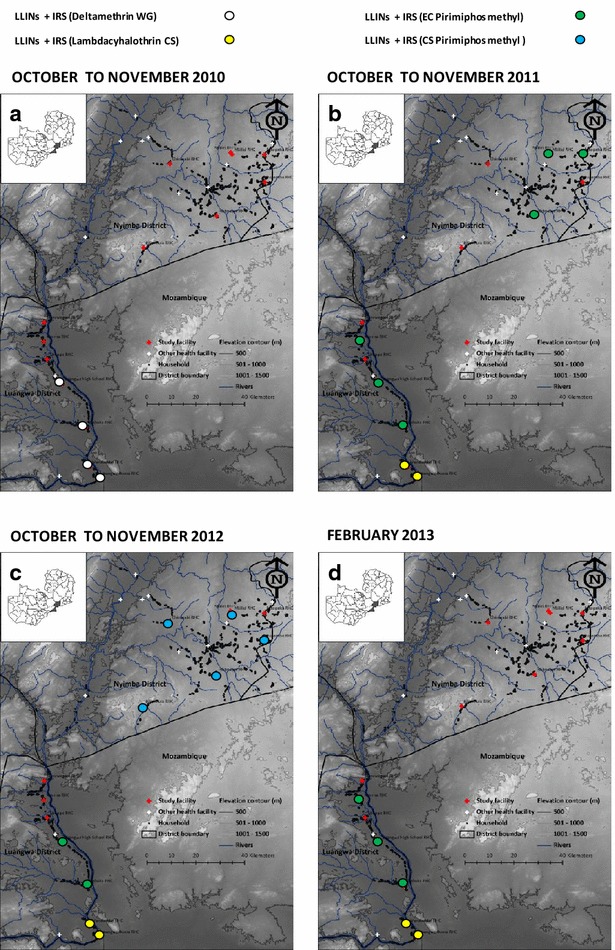
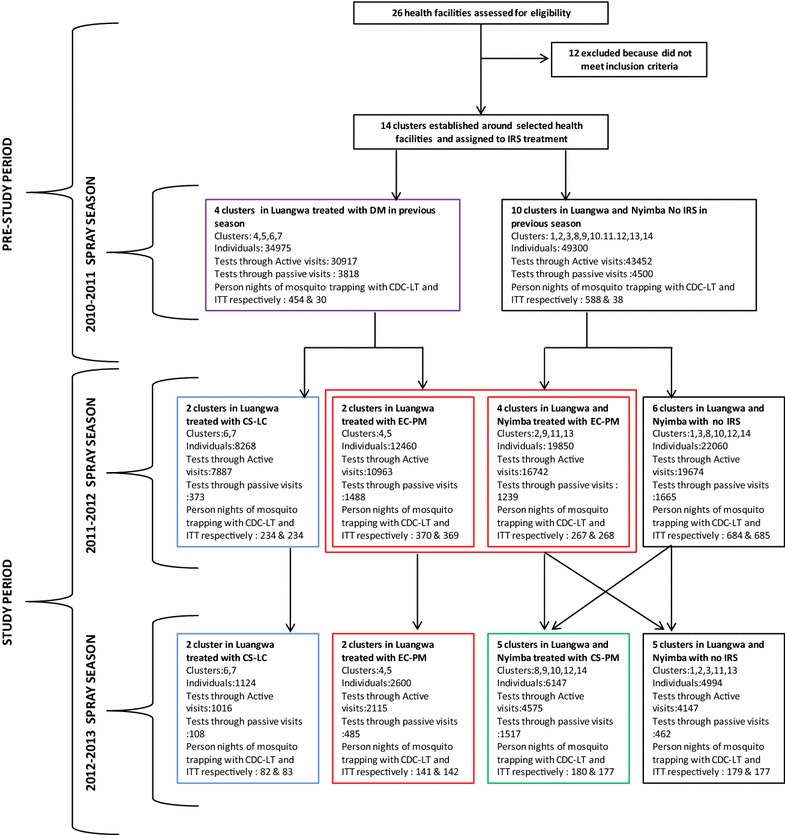
Methods: Fourteen population clusters of approximately 1000 residents each in Zambia's Luangwa and Nyimba districts, which had high pre-existing usage rates (81.7 %) of pyrethroid-impregnated LLINs were quasi-randomly assigned to receive IRS with either of two pyrethroids, namely deltamethrin [Wetable granules (WG)] and lambdacyhalothrin [capsule suspension (CS)], with an emulsifiable concentrate (EC) or CS formulation of the organophosphate pirimiphos methyl (PM), or with no supplementary vector control measure. Diagnostic positivity of patients tested for malaria by community health workers in these clusters was surveyed longitudinally over pre- and post-treatment periods spanning 29 months, over which the treatments were allocated and re-allocated in advance of three sequential rainy seasons.
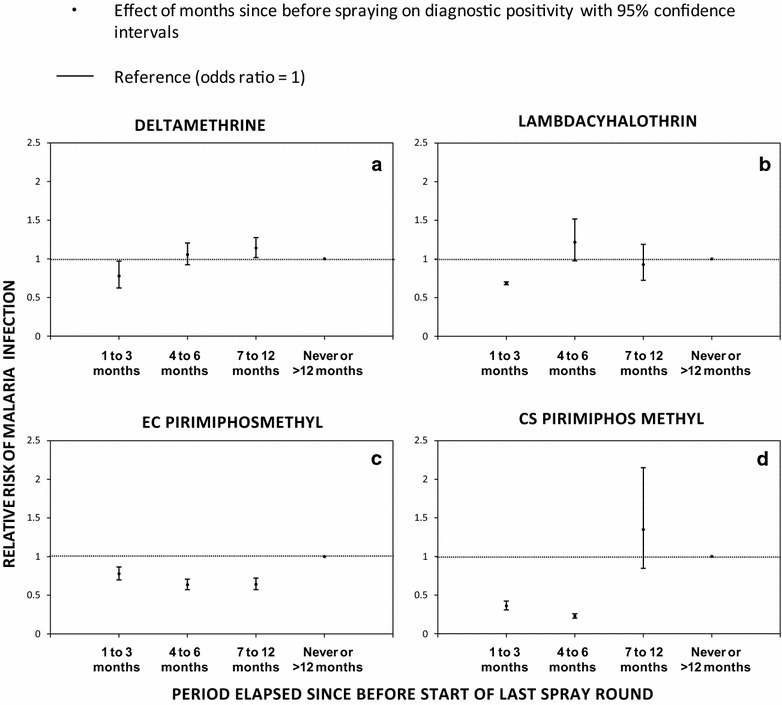
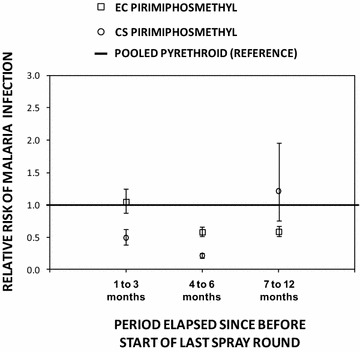
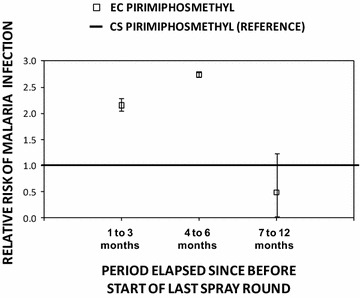
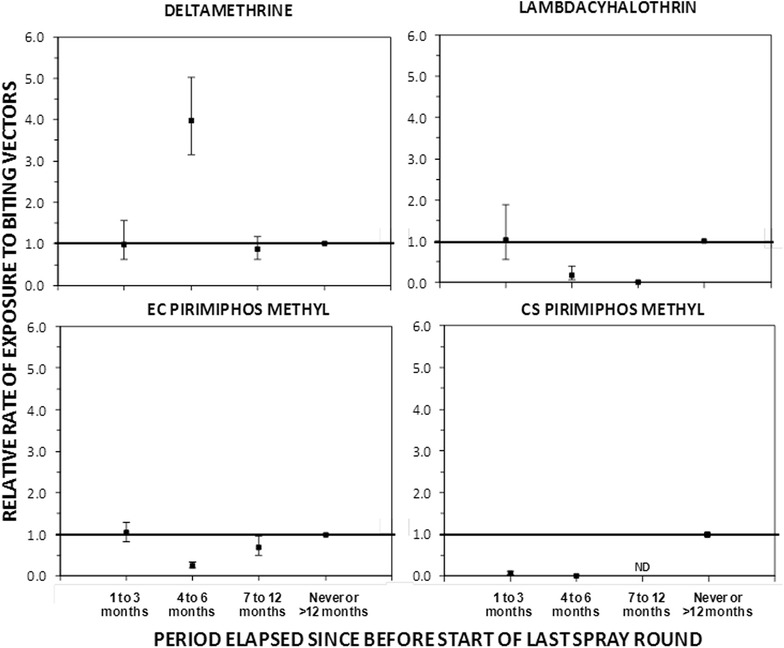
Results: Supplementation of LLINs with PM CS offered the greatest initial level of protection against malaria in the first 3 months of application (incremental protective efficacy (IPE) [95 % confidence interval (CI)] = 0.63 [CI 0.57, 0.69], P < 0.001), followed by lambdacyhalothrin (IPE [95 % CI] = 0.31 [0.10, 0.47], P = 0.006) and PM EC (IPE, 0.23 [CI 0.15, 0.31], P < 0.001) and then by deltamethrin (IPE [95 % CI] = 0.19 [-0.01, 0.35], P = 0.064). Neither pyrethroid formulation provided protection beyond 3 months after spraying, but the protection provided by both PM formulations persisted undiminished for longer periods: 6 months for CS and 12 months for EC. The CS formulation of PM provided greater protection than the combined pyrethroid IRS formulations throughout its effective life IPE [95 % CI] = 0.79 [0.75, 0.83] over 6 months. The EC formulation of PM provided incremental protection for the first 3 months (IPE [95 % CI] = 0.23 [0.15, 0.31]) that was approximately equivalent to the two pyrethroid formulations (lambdacyhalothrin, IPE [95 % CI] = 0.31 [0.10, 0.47] and deltamethrin, IPE [95 % CI] = 0.19 [-0.01, 0.35]) but the additional protection provided by the former, apparently lasted an entire year.
Conclusion: Where universal coverage targets for LLIN utilization has been achieved, supplementing LLINs with IRS using pyrethroids may reduce malaria transmission below levels achieved by LLIN use alone, even in settings where pyrethroid resistance occurs in the vector population. However, far greater reduction of transmission can be achieved under such conditions by supplementing LLINs with IRS using non-pyrethroid insecticide classes, such as organophosphates, so this is a viable approach to mitigating and managing pyrethroid resistance.
Figures
References
-
- WHO. World Malaria Report2012. Geneva: World Health Organization. 2013.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
