

Inhaled corticosteroids and the increased risk of pneumonia: what's new? A 2015 updated review
- PMID: 26893311
- PMCID: PMC5933605
- DOI: 10.1177/1753465816630208
Inhaled corticosteroids and the increased risk of pneumonia: what's new? A 2015 updated review
Abstract
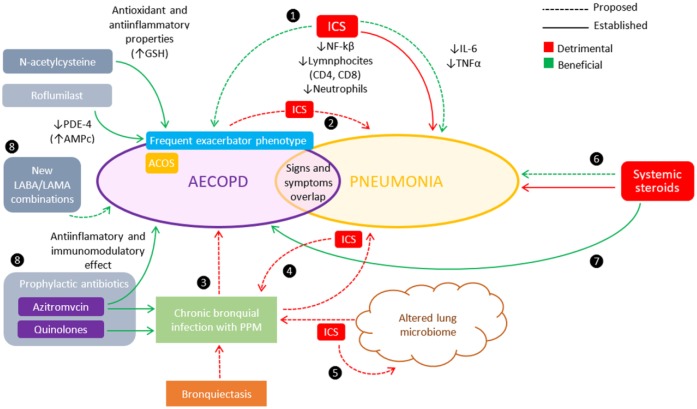
There is a considerable amount of evidence that supports the possibility of an increased risk of pneumonia associated with prolonged use of inhaled corticosteroids (ICS) in patients with chronic obstructive pulmonary disease (COPD). However, as yet, no statistically significant increase in pneumonia-related 30-day mortality in patients on ICS has been demonstrated. The lack of objective pneumonia definitions and radiological confirmations have been a major source of bias, because of the similarities in clinical presentation between pneumonia and acute exacerbations of COPD. One of the newer fluticasone furoate studies overcomes these limitations and also provides an assessment of a range of doses, suggesting that the therapeutic window is quite narrow and that conventional dosing has probably been too high, although the absolute risk may be different compared to other drugs. Newer studies were not able to rule out budesonide as responsible for pneumonia, as previous evidence suggested, and there is still need for evidence from head-to-head comparisons in order to better assess possible intra-class differences. Although the exact mechanisms by which ICS increase the risk of pneumonia are not fully understood, the immunosuppressive effects of ICS on the respiratory epithelium and the disruption of the lung microbiome are most likely to be implicated. Given that COPD represents such a complex and heterogeneous disease, attempts are being made to identify clinical phenotypes with clear therapeutic implications, in order to optimize the pharmacological treatment of COPD and avoid the indiscriminate use of ICS. If deemed necessary, gradual withdrawal of ICS appears to be well tolerated. Vaccination against pneumococcus and influenza should be emphasized in patients with COPD receiving ICS. Physicians should keep in mind that signs and symptoms of pneumonia in COPD patients may be initially indistinguishable from those of an exacerbation, and that patients with COPD appear to be at increased risk of developing pneumonia as a complication of ICS therapy.
Keywords: adverse effects; chronic obstructive pulmonary disease (COPD); inhaled corticosteroids; mortality; phenotypes; pneumonia.
© The Author(s), 2016.
Conflict of interest statement
Figures
References
-
- Agusti A., Fabbri L. (2014) Inhaled steroids in COPD: when should they be used? Lancet Respir Med 2: 869–871. - PubMed
-
- Alcázar Navarrete B., Casanova C., Miravitlles M., de Lucas P., Riesco J., Rodríguez González-Moro J., et al. (2015) “Correct use of inhaled corticosteroids in chronic obstructive pulmonary disease”: a consensus document. Arch Bronconeumol 51: 193–198. - PubMed
-
- Almirall J., Bolibar I., Serra-Prat M., Roig J., Hospital I., Carandell E., et al. (2008) New evidence of risk factors for community-acquired pneumonia: a population-based study. Eur Respir J 31: 1274–1284. - PubMed
-
- Andréjak C., Nielsen R., Thomsen V., Duhaut P., Sørensen H., Thomsen R. (2013) Chronic respiratory disease, inhaled corticosteroids and risk of non-tuberculous mycobacteriosis. Thorax 68: 256–262. - PubMed
-
- Anzueto A., Ferguson G., Feldman G., Chinsky K., Seibert A., Emmett A. (2009) Effect of fluticasone propionate/salmeterol (250/50) on COPD exacerbations and impact on patient outcomes. COPD 6: 320–329. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
