

Subcutaneous Direct-to-Implant Breast Reconstruction: Surgical, Functional, and Aesthetic Results after Long-Term Follow-Up
- PMID: 26893999
- PMCID: PMC4727683
- DOI: 10.1097/GOX.0000000000000533
Subcutaneous Direct-to-Implant Breast Reconstruction: Surgical, Functional, and Aesthetic Results after Long-Term Follow-Up
Abstract
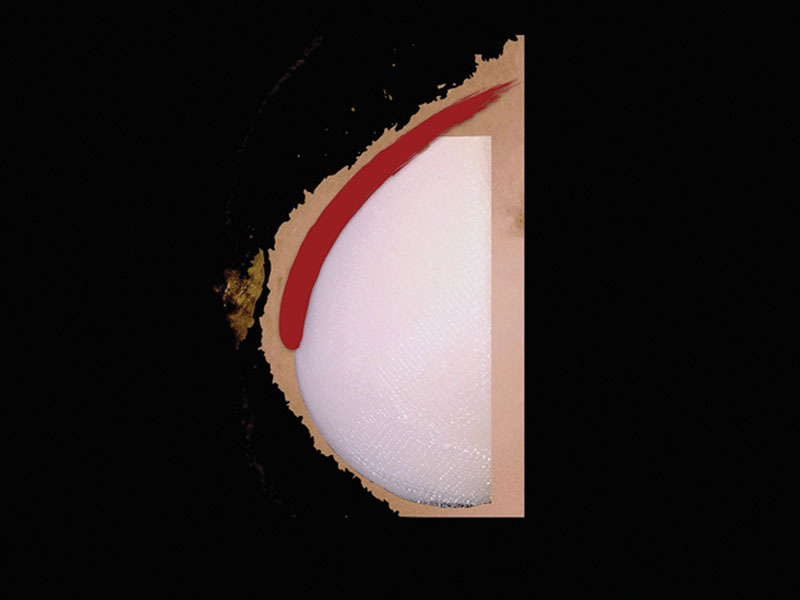
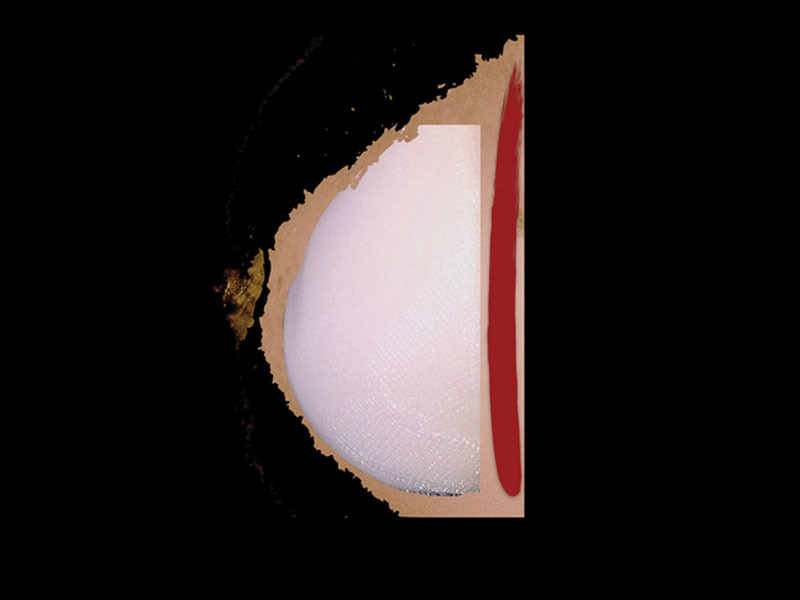
Direct-to-implant breast reconstruction can be achieved more easily by means of soft-tissue replacement devices such as dermal matrices and synthetic meshes. The feasibility of a subcutaneous approach has been recently investigated by some studies with different devices functioning as implant support. Aim of this study is to analyze the long-term results, both objective and subjective, of a previous nonrandomized trial comparing prepectoral (subcutaneous) and retropectoral breast reconstructions.
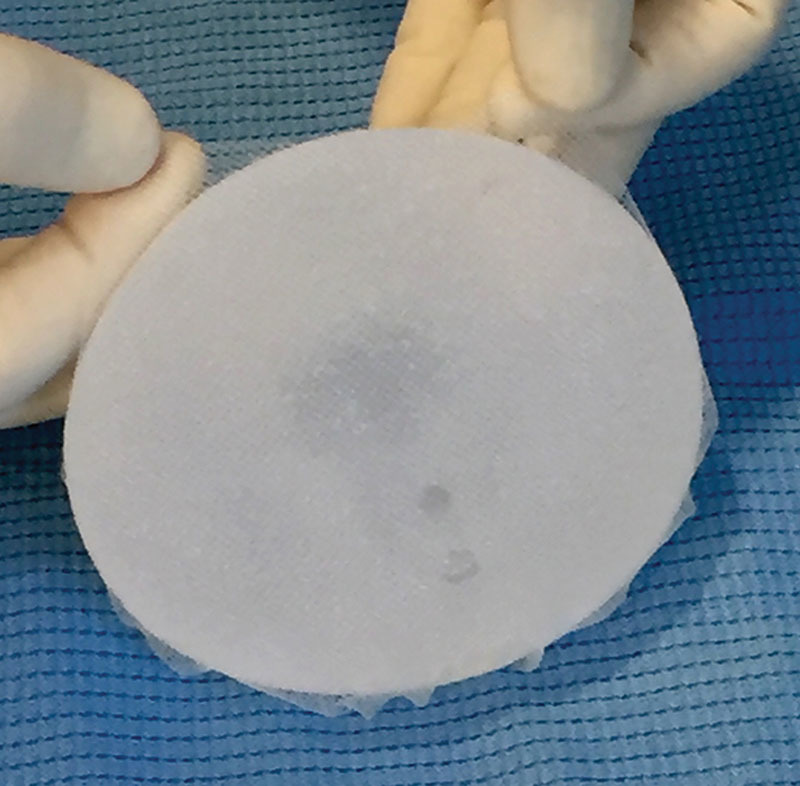
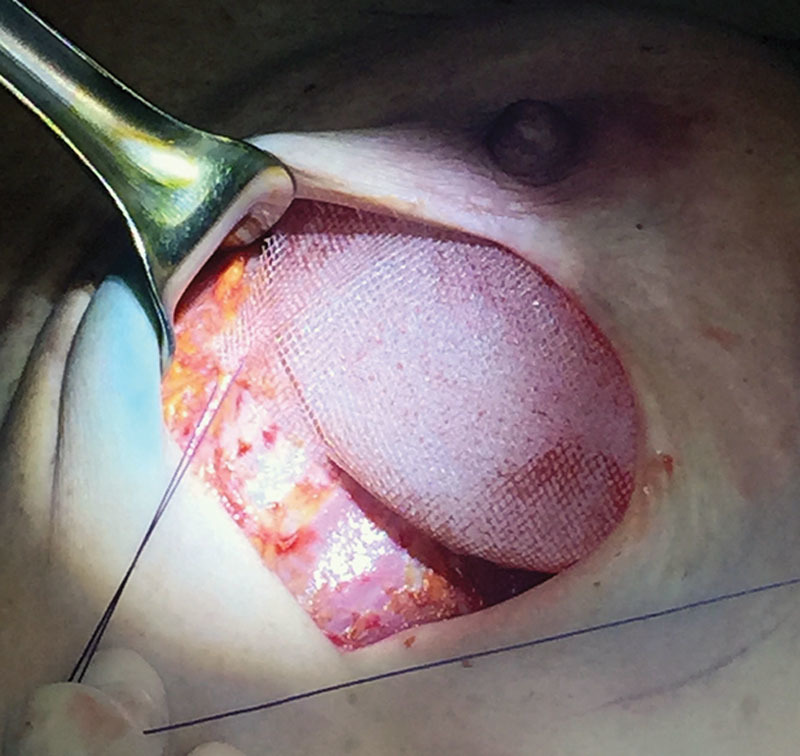
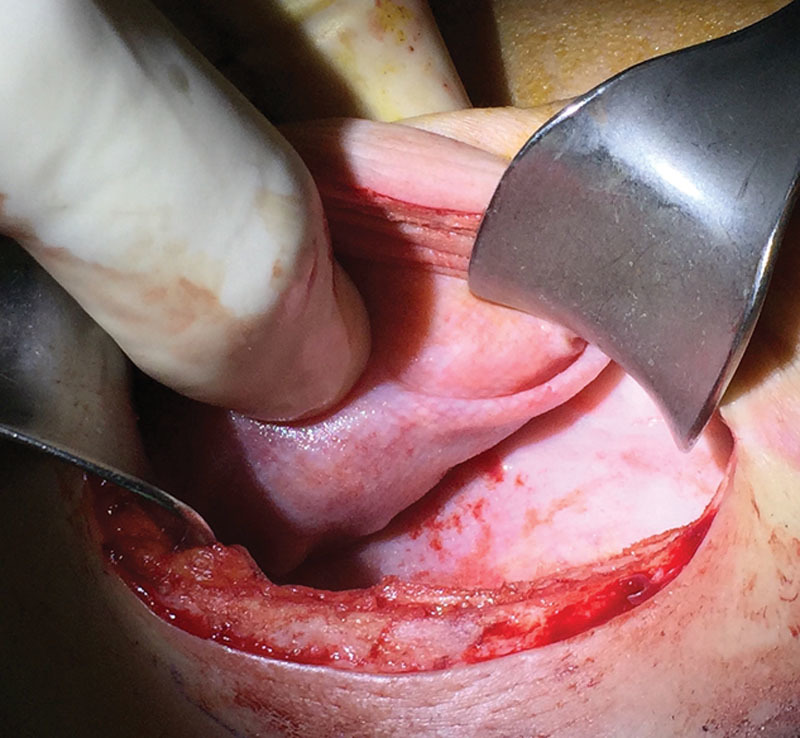
Methods: Patients enrolled in a nonrandomized prospective trial, comparing the standard retropectoral reconstruction and the prepectoral subcutaneous approach, using a titanium-coated mesh in both techniques, were followed up and evaluated for long-term results. Cases were compared in terms of the causes and rate of reinterventions, of the postoperative BREAST-Q questionnaire results, and of an objective surgical evaluation.
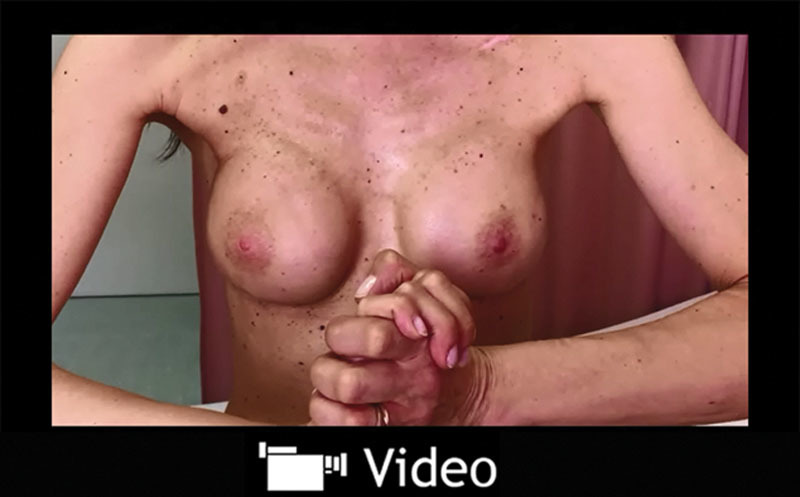
Results: The subcutaneous group had a rate of implant failure and removal of 5.1% when compared with 0% in the retropectoral group. Aesthetic outcome was significantly better for the subcutaneous group both at a subjective and at an objective evaluation. Capsular contracture rate was 0% in the subcutaneous group.
Conclusions: A higher rate of implant failure and removal, although not significant, always because of skin flaps and wound problems, should be taken into account for a careful patients selection. The subcutaneous breast reconstruction shows good long-term results. A coherent subjective and objective cosmetic advantage of this approach emerges. Moreover, no capsular contracture is evident, albeit in a relatively limited number of cases.
Conflict of interest statement
Figures




References
-
- American Society of Plastic Surgeons. Available at: http://www.plasticsurgery.org/Documents/news-resources/statistics/2014-s.... Accessed June 3rd, 2015.
-
- Salzberg CA. Focus on technique: one-stage implant-based breast reconstruction. Plast Reconstr Surg. 2012;130(5 Suppl 2):S95–S103. - PubMed
-
- Kocak E, Nagel TW, Hulsen JH, 3rd, et al. Biologic matrices in oncologic breast reconstruction after mastectomy. Expert Rev Med Devices. 2014;11:65–75. - PubMed
-
- Kim JY, Davila AA, Persing S, et al. A meta-analysis of human acellular dermis and submuscular tissue expander breast reconstruction. Plast Reconstr Surg. 2012;129:28–41. - PubMed
-
- Rawlani V, Buck DW, 2nd, Johnson SA, et al. Tissue expander breast reconstruction using prehydrated human acellular dermis. Ann Plast Surg. 2011;66:593–597. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources