

Commissioning of a motion system to investigate dosimetric consequences due to variability of respiratory waveforms
- PMID: 26894366
- PMCID: PMC5690223
- DOI: 10.1120/jacmp.v17i1.5921
Commissioning of a motion system to investigate dosimetric consequences due to variability of respiratory waveforms
Abstract
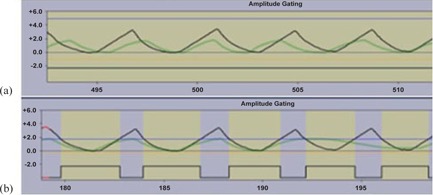
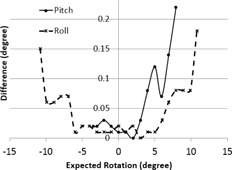
A commercially available six-dimensional (6D) motion system was assessed for accuracy and clinical use in our department. Positional accuracy and respiratory waveform reproducibility were evaluated for the motion system. The system was then used to investigate the dosimetric consequences of respiratory waveform variation when an internal target volume (ITV) approach is used for motion management. The maximum deviations are 0.3 mm and 0.22° for translation and rotation accuracy, respectively, for the tested clinical ranges. The origin reproducibility is less than±0.1 mm. The average differences are less than 0.1 mm with a maximum standard deviation of 0.8 mm between waveforms of actual patients and replication of those waveforms by HexaMotion for three breath-hold and one free-breathing waveform. A modified gamma analysis shows greater than 98% agreement with a 0.5 mm and 100 ms threshold. The motion system was used to investigate respiratory waveform variation and showed that, as the amplitude of the treatment waveform increases above that of the simulation waveform, the periphery of the target volume receives less dose than expected. However, by using gating limits to terminate the beam outside of the simulation amplitude, the results are as expected dosimetrically. Specifically, the average dose difference in the periphery between treating with the simulation waveform and the larger amplitude waveform could be up to 12% less without gating limits, but only differed 2% or less with the gating limits in place. The general functionality of the system performs within the manufacturer's specifications and can accurately replicate patient specific waveforms. When an ITV approach is used for motion management, we found the use of gating limits that coincide with the amplitude of the patient waveform at simulation helpful to prevent the potential underdosing of the target due to changes in patient respiration.
Figures




References
-
- Shah AP, Kupelian PA, Waghorn BJ, et al. Real‐time tumor tracking in the lung using an electromagnetic tracking system. Int J Radiat Oncol Biol Phys. 2013;86(3):477–83. - PubMed
-
- Kubo HD, Len PM, Minohara S, Mostafavi H. Breathing‐synchronized radiotherapy program at the University of California Davis Cancer Center. Med Phys. 2000;27(2):346–53. - PubMed
-
- Ionascu D, Jiang SB, Nishioka S, Shirato H, Berbeco RI. Internal‐external correlation investigations of respiratory induced motion of lung tumors. Med Phys. 2007;34(10):3893–903. - PubMed
-
- Rietzel E, Chen GTY, Choi NC, Willet CG. Four‐dimensional image‐based treatment planning: Target volume segmentation and dose calculation in the presence of respiratory motion. Int J Radiat Oncol Biol Phys. 2005;61(5):1535–50. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
