

Temporal Trends in Hospitalization for Acute Decompensated Heart Failure in the United States, 1998-2011
- PMID: 26895710
- PMCID: PMC4772439
- DOI: 10.1093/aje/kwv455
Temporal Trends in Hospitalization for Acute Decompensated Heart Failure in the United States, 1998-2011
Abstract
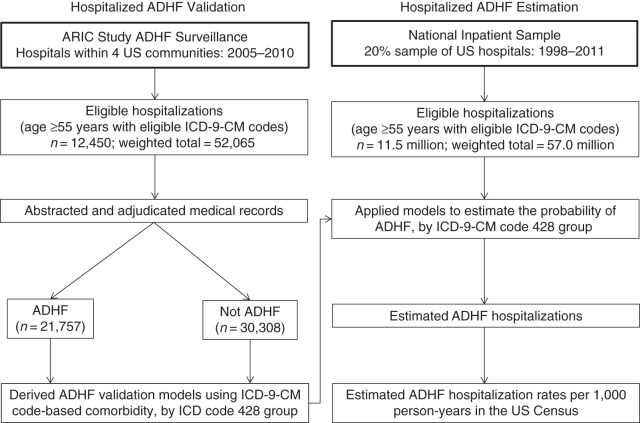
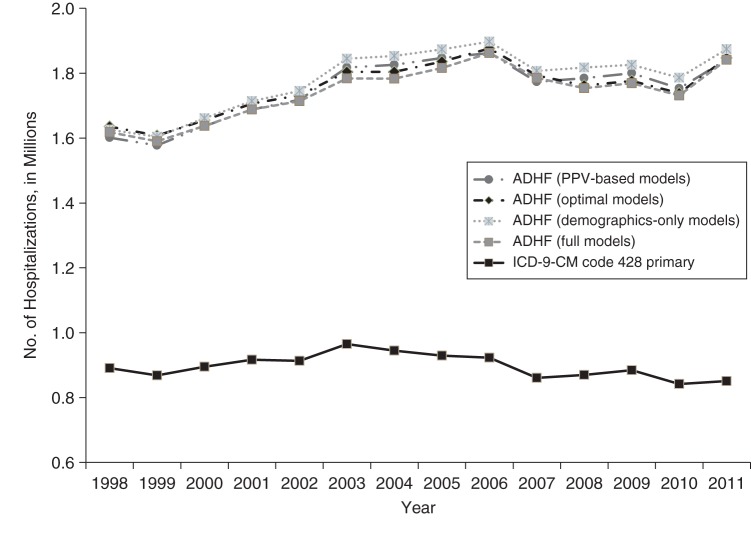
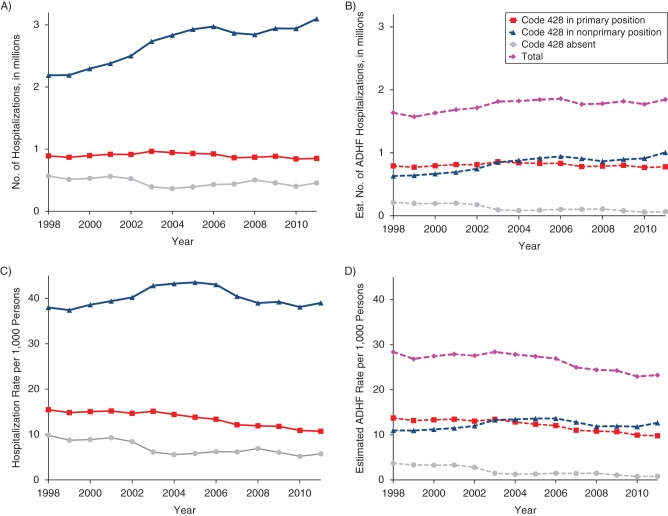
Estimates of the numbers and rates of acute decompensated heart failure (ADHF) hospitalization are central to understanding health-care utilization and efforts to improve patient care. We comprehensively estimated the frequency, rate, and trends of ADHF hospitalization in the United States. Based on Atherosclerosis Risk in Communities (ARIC) Study surveillance adjudicating 12,450 eligible hospitalizations during 2005-2010, we developed prediction models for ADHF separately for 3 International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) code 428 discharge diagnosis groups: 428 primary, 428 nonprimary, or 428 absent. We applied the models to data from the National Inpatient Sample (11.5 million hospitalizations of persons aged ≥55 years with eligible ICD-9-CM codes), an all-payer, 20% probability sample of US community hospitals. The average estimated number of ADHF hospitalizations per year was 1.76 million (428 primary, 0.80 million; 428 nonprimary, 0.83 million; 428 absent, 0.13 million). During 1998-2004, the rate of ADHF hospitalization increased by 2.0%/year (95% confidence interval (CI): 1.8, 2.5) versus a 1.4%/year (95% CI: 0.8, 2.1) increase in code 428 primary hospitalizations (P < 0.001). In contrast, during 2005-2011, numbers of ADHF hospitalizations were stable (-0.5%/year; 95% CI: -1.4, 0.3), while the numbers of 428-primary hospitalizations decreased by -1.5%/year (95% CI: -2.2, -0.8) (P for contrast = 0.03). In conclusion, the estimated number of hospitalizations with ADHF is approximately 2 times higher than the number of hospitalizations with ICD-9-CM code 428 in the primary position. The trend increased more steeply prior to 2005 and was relatively flat after 2005.
Keywords: International Classification of Diseases codes; United States; acute decompensated heart failure; adjudicated heart failure; community surveillance; hospitalizations; national inpatient sample; secular trends.
© The Author 2016. Published by Oxford University Press on behalf of the Johns Hopkins Bloomberg School of Public Health. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures
References
-
- Mozaffarian D, Benjamin EJ, Go AS et al. . Heart disease and stroke statistics—2015 update: a report from the American Heart Association. Circulation. 2015;1314:e29–e322. - PubMed
-
- Dhingra A, Garg A, Kaur S et al. . Epidemiology of heart failure with preserved ejection fraction. Curr Heart Fail Rep. 2014;114:354–365. - PubMed
Publication types
MeSH terms
Grants and funding
- N01 HC055016/HL/NHLBI NIH HHS/United States
- N01 HC055019/HL/NHLBI NIH HHS/United States
- N01-HC-55016/HC/NHLBI NIH HHS/United States
- N01-HC-55021/HC/NHLBI NIH HHS/United States
- N01 HC055020/HL/NHLBI NIH HHS/United States
- N01-HC-55019/HC/NHLBI NIH HHS/United States
- N01-HC-55015/HC/NHLBI NIH HHS/United States
- N01-HC-55020/HC/NHLBI NIH HHS/United States
- T32HL007024/HL/NHLBI NIH HHS/United States
- N01 HC055018/HL/NHLBI NIH HHS/United States
- N01 HC055022/HL/NHLBI NIH HHS/United States
- N01-HC-55018/HC/NHLBI NIH HHS/United States
- N01-HC-55022/HC/NHLBI NIH HHS/United States
- N01 HC055021/HL/NHLBI NIH HHS/United States
- T32 HL007024/HL/NHLBI NIH HHS/United States
- N01 HC055015/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
