

"Nihilism" of chronic heart failure therapy in children and why effective therapy is withheld
- PMID: 26895877
- PMCID: PMC4806719
- DOI: 10.1007/s00431-016-2700-3
"Nihilism" of chronic heart failure therapy in children and why effective therapy is withheld
Abstract
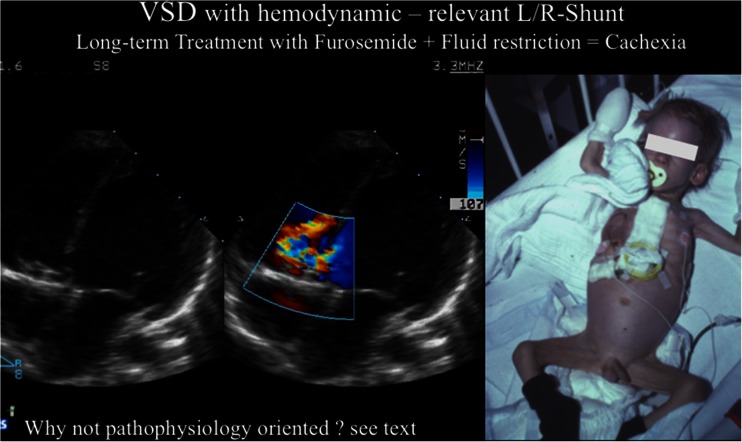
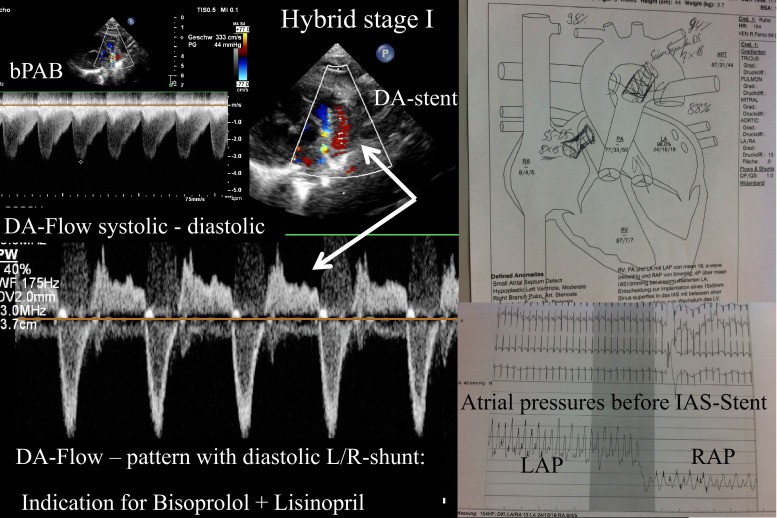
Major advances in chronic heart failure (cHF) therapy have been achieved and documented in adult patients, while research regarding the mechanisms and therapy of cHF in children has lagged behind. Based on receptor physiological studies and pharmacological knowledge, treatment with specific ß1-adrenergic receptor blocker (ARB), tissue angiotensin-converting enzyme inhibitor (ACE-I), and mineralocorticoid antagonists have to be recommended in children despite lack of sufficient data derived from prospective randomized studies. At our institution, bisoprolol, lisinopril, and spironolactone have been firmly established to treat systolic cHF, hypoplastic left heart syndrome (HLHS) following hybrid approach and congenital left-right shunt diseases, latest in patients where surgery has to be delayed. Chronic therapy with long-acting diuretics and fluid restriction are not advocated because short-term effects are achieved at the expense of further neuro-humoral stimulation. It remains unclear why diuretics are recommended although evidence-based studies, documenting long-term benefit, are missing. However, that is true for all currently used drugs for pediatric cHF.
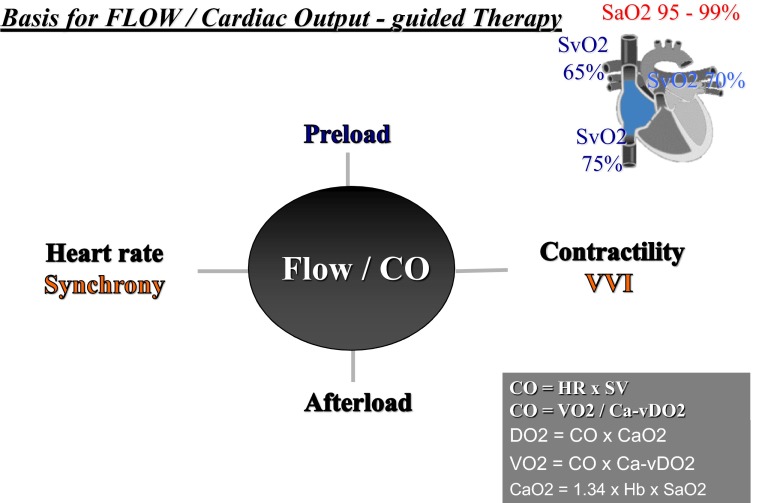
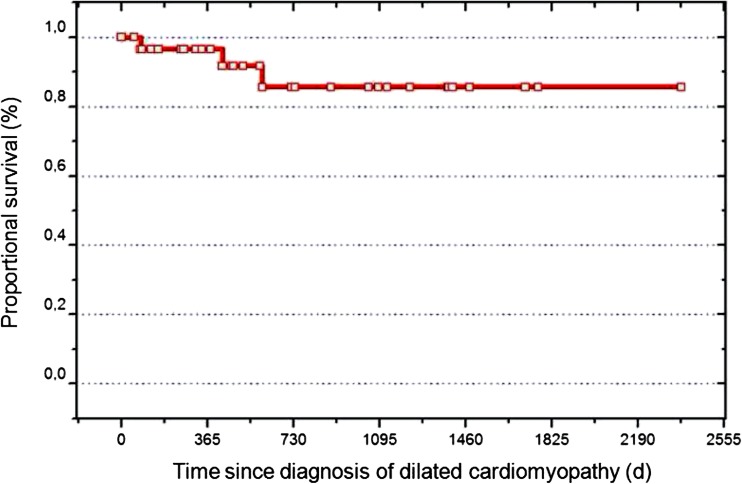
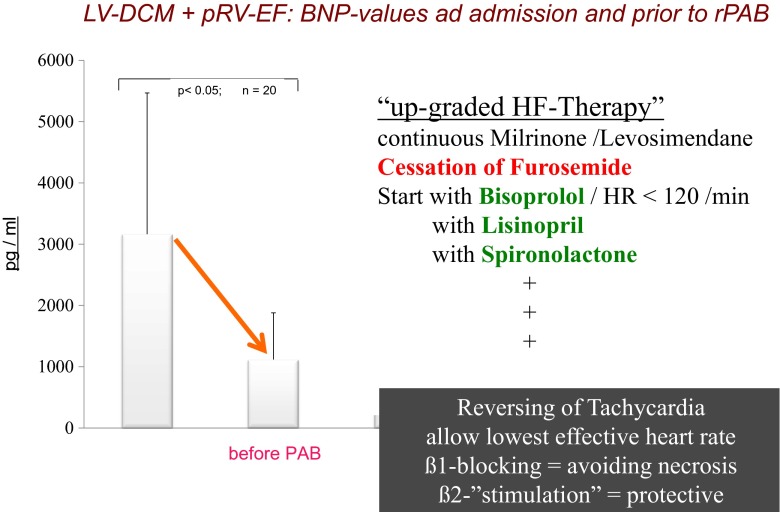
Conclusion: This review focuses on the prevailing "nihilism" of cHF therapy in children with the goal to encourage physicians to treat pediatric cHF with a rationally designed therapy, which combines available agents that have been shown to improve survival in adult patients with cHF. Because of the lack of clinical trials, which generate the needed evidence, surrogate variables like heart and respiratory rate, weight gain, image-derived data, and biomarkers should be monitored and used instead. The recommended pharmacological therapy for systolic heart failure is also provided as the basis for utilizing reversible pulmonary arterial banding (PAB) as a novel strategy in young children with dilative cardiomyopathy (DCM) with preserved right ventricular function.
What is known: • Heart failure (HF) in children is a serious public health concern. • HF has numerous etiologies, but unspecific symptoms. • HF interplays among neuro-humoral, and molecular abnormalities. • Pediatric cHF-therapy is currently based on loop-diuretics, fluid restriction and digoxin. What is New: • Cardiac function analysis has to include cardiac synchrony and VVI. • Considering enormous potential of cardiac regeneration, therapy has to extend with selective ß1-ARB, tissue ACE-I and mineralocorticoid blockers, loop-diuretics avoided as ever possible. • Inhibition of the endogenous neuro-humoral stimulation is monitored by surrogate parameters as heart and breath rate and systolic and diastolic blood pressure. • Advocated HF therapy serves for regenerative strategies as reversible Pulmonary Artery Banding in DCM.
Keywords: Bisoprolol; Chronic heart failure; Infants and children; Lisinopril; Pulmonary artery banding; Spironolactone.
Figures
References
-
- (1987) Effects of enalapril on mortality in severe congestive heart failure. Results of the Cooperative North Scandinavian Enalapril Survival Study (CONSENSUS). The aldosterone CONSENSUS Trial Study Group. N Engl J Med 316:1429–1435 - PubMed
-
- (1999) Effect of metoprolol CR/XL in chronic heart failure: metoprolol CR/XL Randomized Intervention Trial in Congestive Heart Failure (MERIT-HF). Lancet 353:2001–2007 - PubMed
-
- (1999) The Cardiac Insufficiency Bisoprolol Study II (CIBIS-II): a randomized trial. Lancet 353: 9–13 - PubMed
-
- Ahmet I, Krawczyk M, Zhu W, Woo AY, Morrell C, Poosala S, Xiao RP, Lakatta EG, Talan MI. Cardioprotective and survival benefits of long-term combined therapy with beta2 adrenoreceptor (AR) agonist and beta1 AR blocker in dilated cardiomyopathy postmyocardial infarction. J Pharmacol Exp Ther. 2008;325:491–499. doi: 10.1124/jpet.107.135335. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
