

Diagnostic accuracy of staging laparoscopy for detecting metastasized or locally advanced perihilar cholangiocarcinoma: a systematic review and meta-analysis
- PMID: 26895909
- PMCID: PMC5009158
- DOI: 10.1007/s00464-016-4788-y
Diagnostic accuracy of staging laparoscopy for detecting metastasized or locally advanced perihilar cholangiocarcinoma: a systematic review and meta-analysis
Abstract
Background: Despite extensive preoperative staging, still almost half of patients with potentially resectable perihilar cholangiocarcinoma (PHC) have locally advanced or metastasized disease upon exploratory laparotomy. The value of routine staging laparoscopy (SL) in these patients remains unclear with varying results reported in the literature. The aim of the present systematic review was to provide an overview of studies on SL in PHC and to define its current role in preoperative staging.
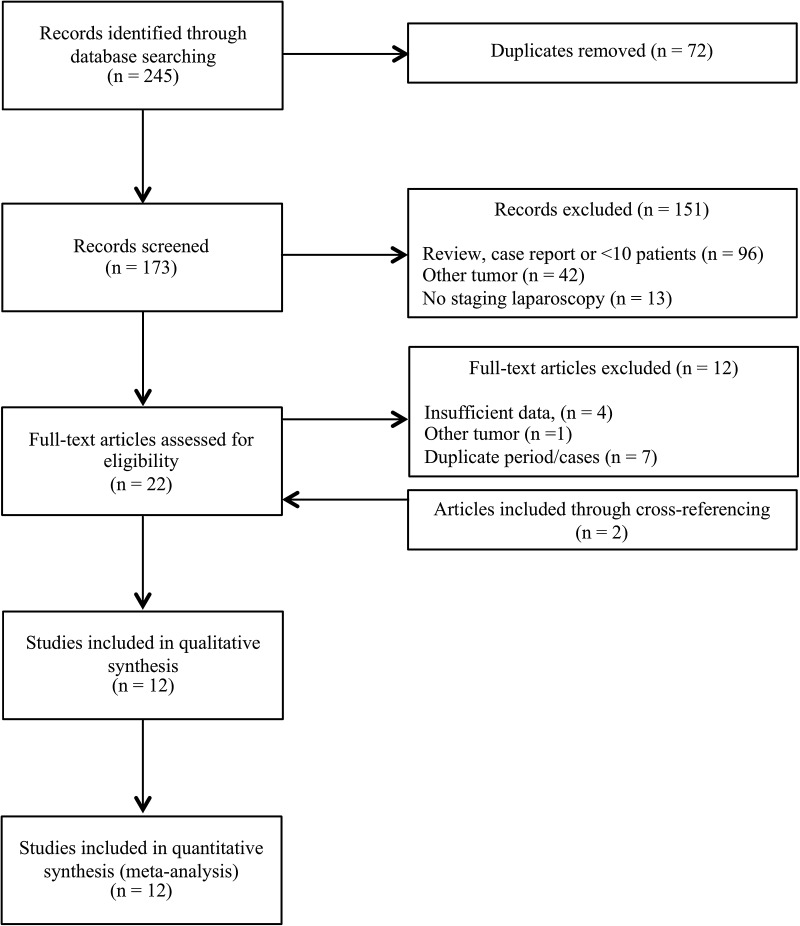
Methods: A systematic review and meta-analysis were performed in PubMed and EMBASE regarding studies providing data on the diagnostic accuracy of SL in PHC. Primary outcome measures were the overall yield and sensitivity to detect unresectable disease. Secondary outcomes were the yield and sensitivity for recent studies (after 2010) and large study cohorts (≥100 patients) and specific (metastatic) lesions. Methodological quality of studies was assessed with the Quality Assessment of Diagnostic Accuracy Studies tool.
Results: From 173 records, 12 studies including 832 patients met the inclusion criteria. The yield of SL in PHC varied from 6.4 to 45.0 % with a pooled yield of 24.4 % [95 % confidence interval (CI) 16.4-33.4]. Sensitivity to detect unresectable disease ranged from 31.6 to 75 % with a pooled sensitivity of 52.2 % (95 % CI 47.1-57.2). Sensitivity was highest for peritoneal metastases (80.7 %, 95 % CI 70.9-88.3). Subgroup analysis revealed that the yield and sensitivity tended to be lower for studies after 2010. Considerable heterogeneity was detected among the studies.
Conclusions: The results of the pooled analyses suggest that one in four patients with potentially resectable PHC benefits from SL. Given considerable heterogeneity, a trend to lower yield in more recent studies and further improvement of preoperative imaging over time, the routine use of SL seems discouraging. Studies that identify predictors of unresectability, that enable selection of patients who will benefit the most from this procedure, are needed.
Keywords: Diagnostic accuracy; Perihilar cholangiocarcinoma; Resectability; Staging laparoscopy; Yield.
Conflict of interest statement
Compliance with ethical standards Disclosures No financial grants or other fundings have been received in support of this study. The authors, Robert J. S. Coelen, Anthony T. Ruys, Marc G. H. Besselink, Olivier R. C. Busch and Thomas M. van Gulik, declare no conflict of interest.
Figures




Similar articles
-
Diagnostic accuracy of laparoscopy following computed tomography (CT) scanning for assessing the resectability with curative intent in pancreatic and periampullary cancer.Cochrane Database Syst Rev. 2016 Jul 6;7(7):CD009323. doi: 10.1002/14651858.CD009323.pub3. Cochrane Database Syst Rev. 2016. PMID: 27383694 Free PMC article.
-
The value of FDG positron emission tomography/computerised tomography (PET/CT) in pre-operative staging of colorectal cancer: a systematic review and economic evaluation.Health Technol Assess. 2011 Sep;15(35):1-192, iii-iv. doi: 10.3310/hta15350. Health Technol Assess. 2011. PMID: 21958472 Free PMC article.
-
Lymph node dissection in resectable perihilar cholangiocarcinoma: a systematic review.Am J Surg. 2015 Oct;210(4):694-701. doi: 10.1016/j.amjsurg.2015.05.015. Epub 2015 Jun 29. Am J Surg. 2015. PMID: 26212390
-
Positron emission tomography (PET) and magnetic resonance imaging (MRI) for the assessment of axillary lymph node metastases in early breast cancer: systematic review and economic evaluation.Health Technol Assess. 2011 Jan;15(4):iii-iv, 1-134. doi: 10.3310/hta15040. Health Technol Assess. 2011. PMID: 21276372 Free PMC article.
-
Development of a Risk Score to Predict Detection of Metastasized or Locally Advanced Perihilar Cholangiocarcinoma at Staging Laparoscopy.Ann Surg Oncol. 2016 Dec;23(Suppl 5):904-910. doi: 10.1245/s10434-016-5531-6. Epub 2016 Sep 1. Ann Surg Oncol. 2016. PMID: 27586005 Free PMC article.
Cited by
-
Surgical Therapy for Perihilar Cholangiocarcinoma: State of the Art.Visc Med. 2021 Feb;37(1):18-25. doi: 10.1159/000514032. Epub 2021 Jan 7. Visc Med. 2021. PMID: 33708815 Free PMC article. Review.
-
Current Perspectives on the Surgical Management of Perihilar Cholangiocarcinoma.Cancers (Basel). 2022 Apr 28;14(9):2208. doi: 10.3390/cancers14092208. Cancers (Basel). 2022. PMID: 35565335 Free PMC article. Review.
-
Impact of Positive Lymph Nodes and Resection Margin Status on the Overall Survival of Patients with Resected Perihilar Cholangiocarcinoma: The ENSCCA Registry.Cancers (Basel). 2022 May 12;14(10):2389. doi: 10.3390/cancers14102389. Cancers (Basel). 2022. PMID: 35625993 Free PMC article.
-
Optimal perioperative care in peri-hilar cholangiocarcinoma resection.Eur Surg. 2018;50(3):93-99. doi: 10.1007/s10353-018-0529-x. Epub 2018 May 4. Eur Surg. 2018. PMID: 29875797 Free PMC article.
-
Preoperative predictors for non-resectability in perihilar cholangiocarcinoma.World J Surg Oncol. 2024 Feb 7;22(1):48. doi: 10.1186/s12957-024-03329-1. World J Surg Oncol. 2024. PMID: 38326854 Free PMC article.
References
-
- Matsuo K, Rocha FG, Ito K, D’Angelica MI, Allen PJ, Fong Y, Dematteo RP, Gonen M, Endo I, Jarnagin WR. The Blumgart preoperative staging system for hilar cholangiocarcinoma: analysis of resectability and outcomes in 380 patients. J Am Coll Surg. 2012;215:343–355. doi: 10.1016/j.jamcollsurg.2012.05.025. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
