

Decellularized aortic homografts for aortic valve and aorta ascendens replacement
- PMID: 26896320
- PMCID: PMC4913875
- DOI: 10.1093/ejcts/ezw013
Decellularized aortic homografts for aortic valve and aorta ascendens replacement
Abstract
Objectives: The choice of valve prosthesis for aortic valve replacement (AVR) in young patients is challenging. Decellularized pulmonary homografts (DPHs) have shown excellent results in pulmonary position. Here, we report our early clinical results using decellularized aortic valve homografts (DAHs) for AVR in children and mainly young adults.
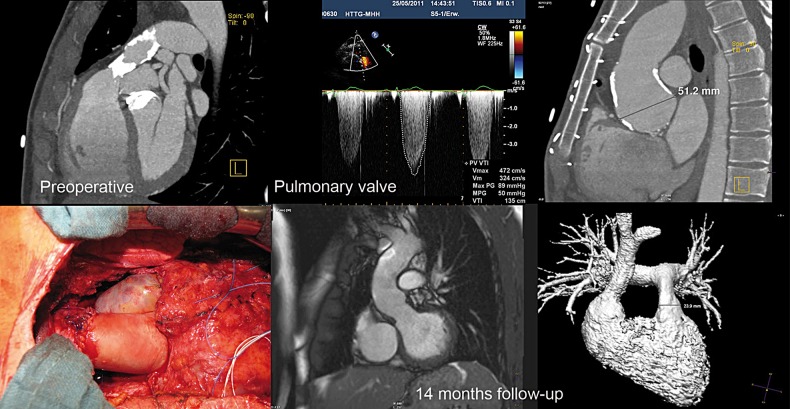
Methods: This prospective observational study included all 69 patients (44 males) operated from February 2008 to September 2015, with a mean age of 19.7 ± 14.6 years (range 0.2-65.3 years). In 18 patients, a long DAH was used for simultaneous replacement of a dilated ascending aorta as an extended aortic root replacement (EARR). Four patients received simultaneous pulmonary valve replacement with DPH.
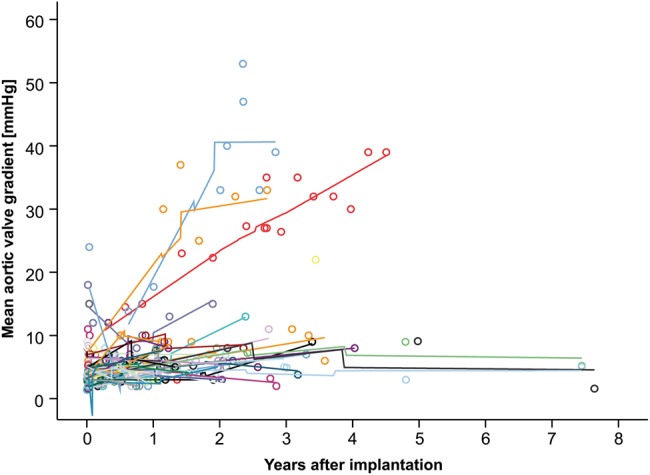
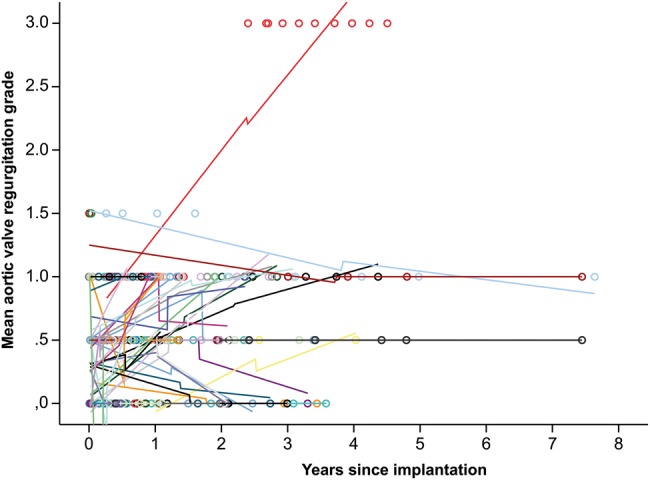
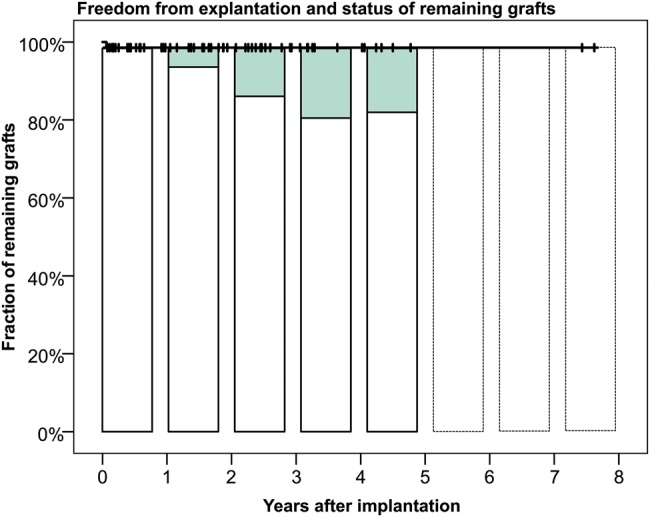
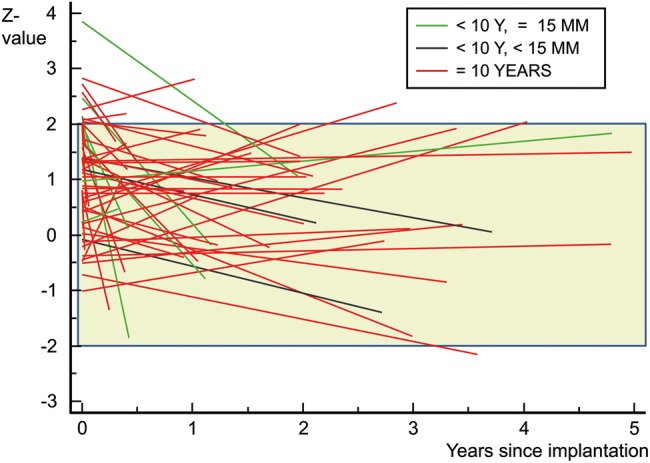
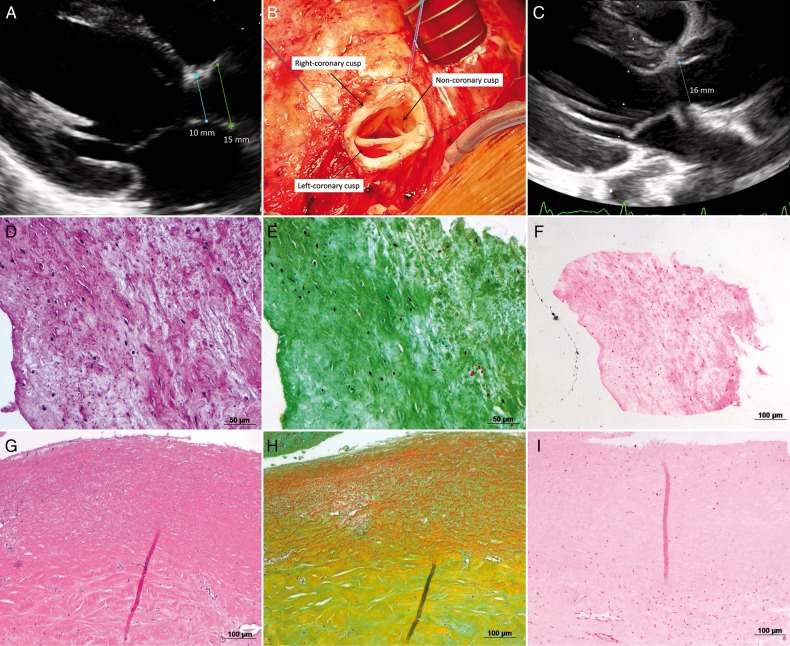
Results: Thirty-nine patients (57%) had a total of 62 previous operations. The mean aortic cross-clamp time in isolated cases was 129 ± 41 min. There was 1 conduit-unrelated death. The mean DAH diameter was 22.4 ± 3.7 mm (range, 10-29 mm), the average peak gradient was 14 ± 15 mmHg and the mean aortic regurgitation grade (0.5 = trace, 1 = mild) was 0.6 ± 0.5. The mean effective orifice area (EOA) of 25 mm diameter DAH was 3.07 ± 0.7 cm(2). DAH annulus z-values were 1.1 ± 1.1 at implantation and 0.7 ± 1.3 at the last follow-up. The last mean left ventricle ejection fraction and left ventricle end diastolic volume index was 63 ± 7% and 78 ± 16 ml/m(2) body surface area, respectively. To date, no dilatation has been observed at any level of the graft during follow-up; however, the observational time is short (140.4 years in total, mean 2.0 ± 1.8 years, maximum 7.6 years). One small DAH (10 mm at implantation) had to be explanted due to subvalvular stenosis and developing regurgitation after 4.5 years and was replaced with a 17 mm DAH without complication. No calcification of the explanted graft was noticed intraoperatively and after histological analysis, which revealed extensive recellularization without inflammation.
Conclusions: DAHs withstand systemic circulation, provide outstanding EOA and appear as an alternative to conventional grafts for AVR in young patients. EARR using DAH is a further option in aortic valve disease associated with aorta ascendens dilatation as it avoids the use of any prosthetic material.
Keywords: Aortic valve; Decellularized homografts; Valve prosthesis; Valve replacement.
© The Author 2016. Published by Oxford University Press on behalf of the European Association for Cardio-Thoracic Surgery.
Figures
References
-
- Siregar S, de Heer F, Groenwold RH, Versteegh MI, Bekkers JA, Brinkman ES et al. . Trends and outcomes of valve surgery: 16-year results of The Netherlands Cardiac Surgery National Database. Eur J Cardiothorac Surg 2014;46:386–97. - PubMed
-
- Beckmann A, Funkat AK, Lewandowski J, Frie M, Schiller W, Hekmat K et al. . Cardiac surgery in Germany during 2012: a report on behalf of the German Society for Thoracic and Cardiovascular Surgery. J Thorac Cardiovasc Surg 2014;62:5–17. - PubMed
-
- Bouhout I, Stevens LM, Mazine A, Poirier N, Cartier R, Demers P et al. . Long-term outcomes after elective isolated mechanical aortic valve replacement in young adults. J Thorac Cardiovasc Surg 2014;148:1341–6. e1. - PubMed
-
- Kalfa D, Mohammadi S, Kalavrouziotis D, Kharroubi M, Doyle D, Marzouk M et al. . Long-term outcomes of the Ross procedure in adults with severe aortic stenosis: single-centre experience with 20 years of follow-up. Eur J Cardiothoracic Surg 2015;47:159–67. - PubMed
-
- Andreas M, Wiedemann D, Seebacher G, Rath C, Aref T, Rosenhek R et al. . The Ross procedure offers excellent survival compared with mechanical aortic valve replacement in a real-world setting. Eur J Cardiothoracic Surg 2014;46:409–13. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
