

Efficacy of axillary exclusion on seroma formation after modified radical mastectomy
- PMID: 26897384
- PMCID: PMC4761189
- DOI: 10.1186/s12957-016-0801-0
Efficacy of axillary exclusion on seroma formation after modified radical mastectomy
Abstract
Background: Breast cancer represented 35.1% of total female cancer cases in Egypt. Seroma is one of the most serious and common complications of mastectomy and axillary dissection with incidence between 15 and 81%. Seroma formation delays wound healing and increases susceptibility to infection, skin flap necrosis, and persistent pain as well as prolonging convalescence. Therefore, several techniques have been investigated to minimize seroma formation with no consistent success. Axillary exclusion is a technique aimed to obliterate dead space after axillary clearance and minimize collection.
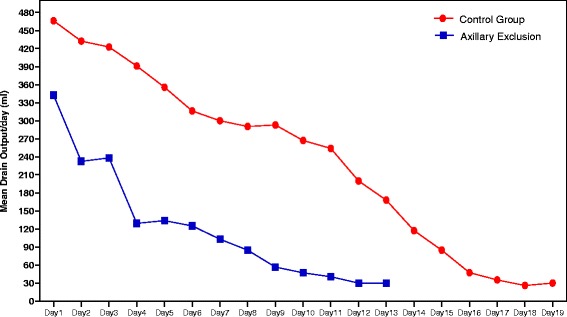
Methods: Sixty-four patients were prepared for modified radical mastectomy. Of those, the study group contains 32 patients and the control group contains 32 patients. Study group had axillary exclusion while the other had the conventional procedure; total drain outputs were recorded daily for all patients prior to drain removal. The drains were removed when the daily drainage was less than 30 ml.
Results: This study contains 64 patients, the study group contains 32 patients, and the control group contains 32 patients. Age, BMI (mean control=31.7 and study=30.2), and tumor size were of no significant differences to be more concise on the effect of axillary exclusion. The mean of day of drain removal in the control group was 17.8 day (15-19) with a mean of total drain output of 4525.6 ml (4430-3660 ml) while the mean in the study group of day of drain removal was 11.3 (10-13) with a mean of total drain output of 1476.2 ml (620-2200 ml), p<0.00.
Conclusions: Axillary exclusion technique is a valuable procedure that significantly decreases seroma postmastectomy and axillary dissection.
Figures


References
-
- Ozdoğan M, Yılmaz KB, Ozaslan C, Gurer A, Gulbahar O, Ersoy E. Scalpel versus electrocautery dissections: the effect on wound complications and pro-inflammatory cytokine levels in wound fluid. Turk J Med Sci. 2008;38:111–116.
-
- Hokkam E, Farrag S, El Kammash S. Tetracycline sclerotherapy in treating postmastectomy seroma: a simple solution for a frequently occurring problem. Egyptian J Surgery. 2009;28:99–104.
-
- Kuroi K, Shimozuma K, Taguchi T, Imai H, Yamashiro H, Ohsumi S, et al. Evidence-based risk factors for seroma formation in breast surgery. Clin Oncol. 2006;36(4):197–206. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
