

The value of vital sign trends for detecting clinical deterioration on the wards
- PMID: 26898412
- PMCID: PMC4834231
- DOI: 10.1016/j.resuscitation.2016.02.005
The value of vital sign trends for detecting clinical deterioration on the wards
Abstract
Aim: Early detection of clinical deterioration on the wards may improve outcomes, and most early warning scores only utilize a patient's current vital signs. The added value of vital sign trends over time is poorly characterized. We investigated whether adding trends improves accuracy and which methods are optimal for modelling trends.
Methods: Patients admitted to five hospitals over a five-year period were included in this observational cohort study, with 60% of the data used for model derivation and 40% for validation. Vital signs were utilized to predict the combined outcome of cardiac arrest, intensive care unit transfer, and death. The accuracy of models utilizing both the current value and different trend methods were compared using the area under the receiver operating characteristic curve (AUC).
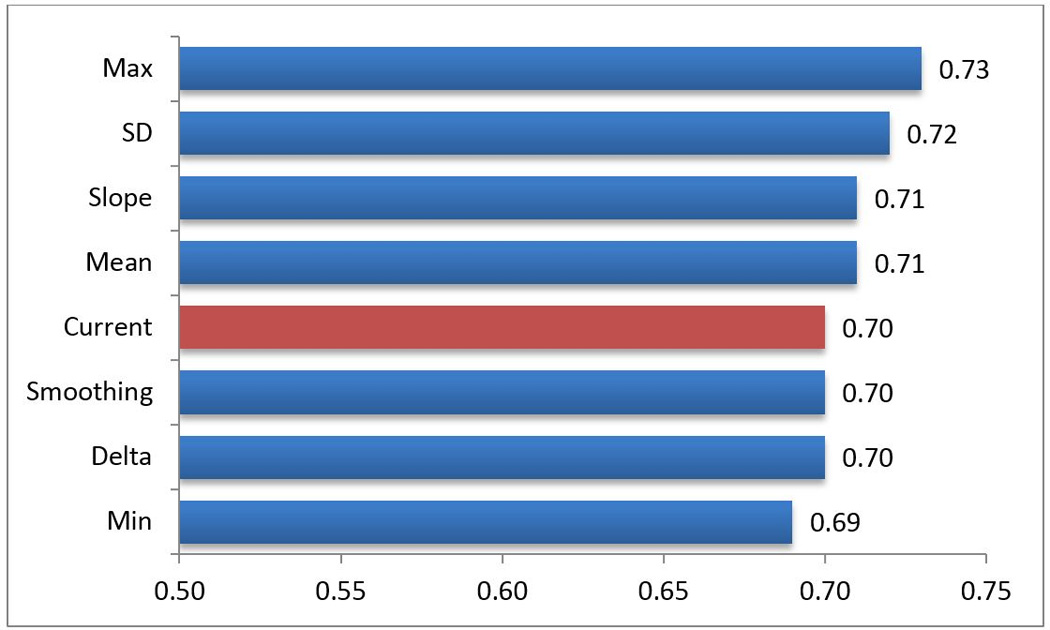
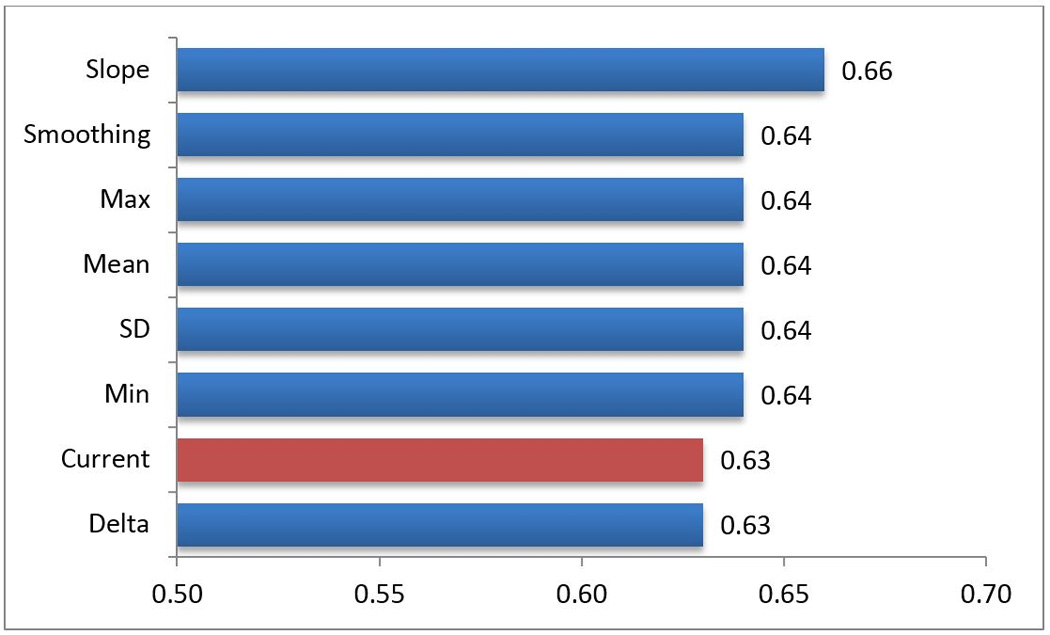
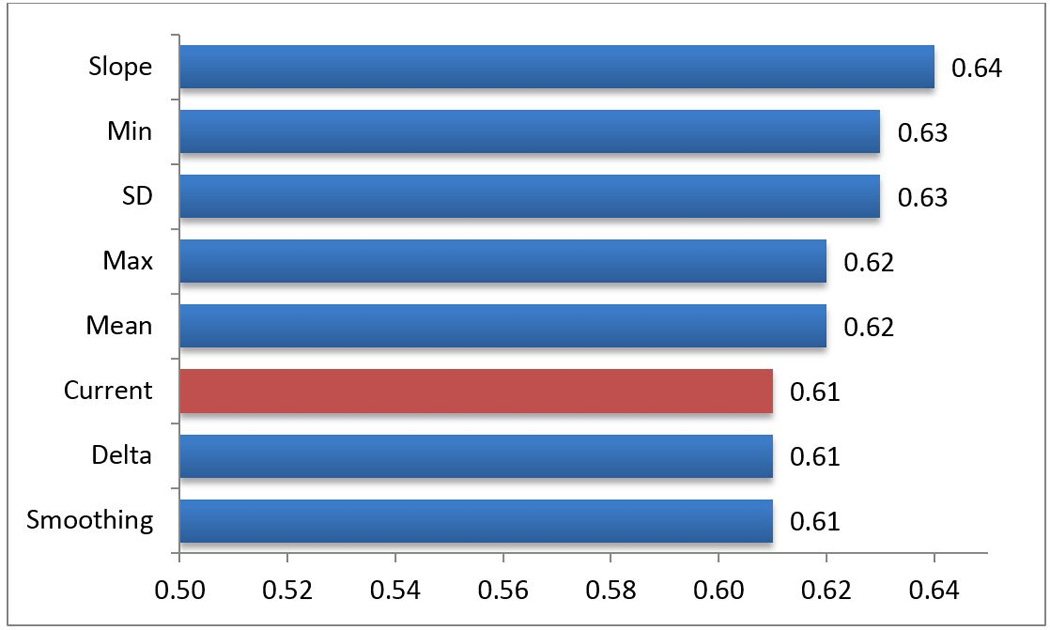
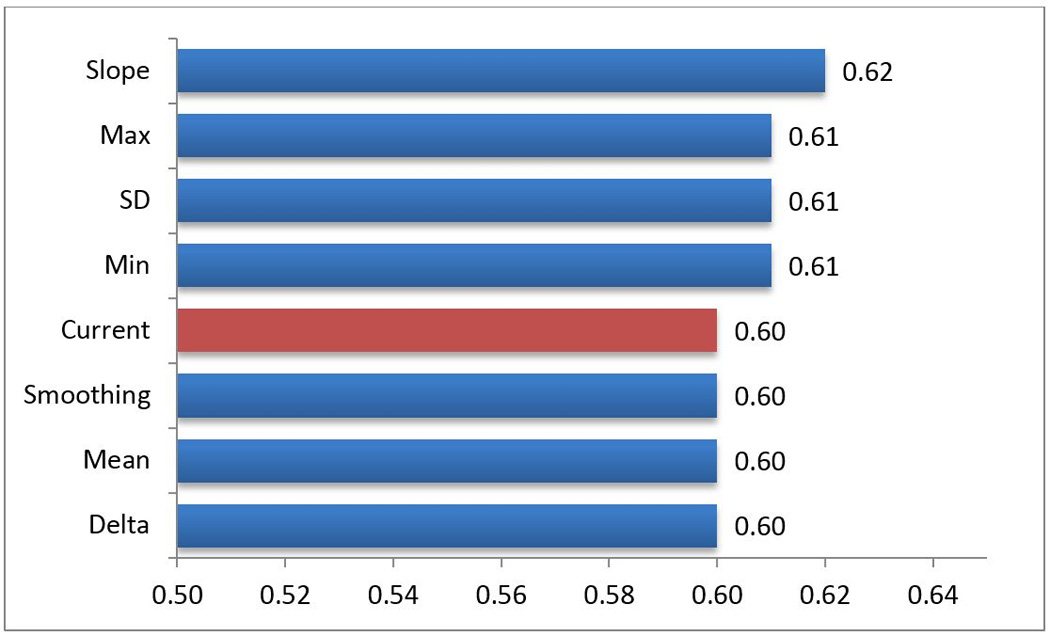
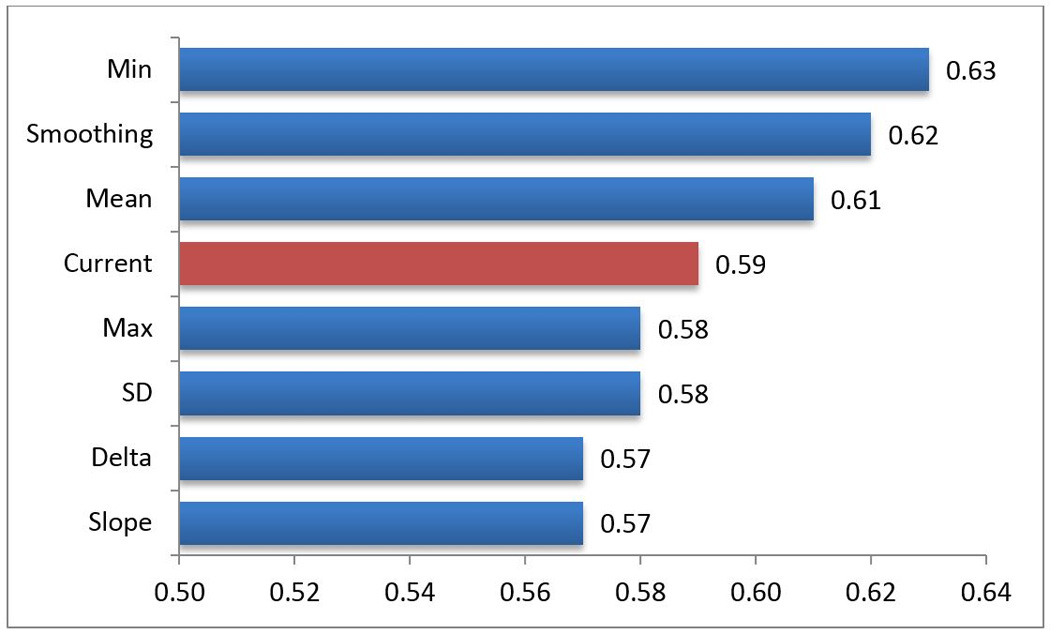
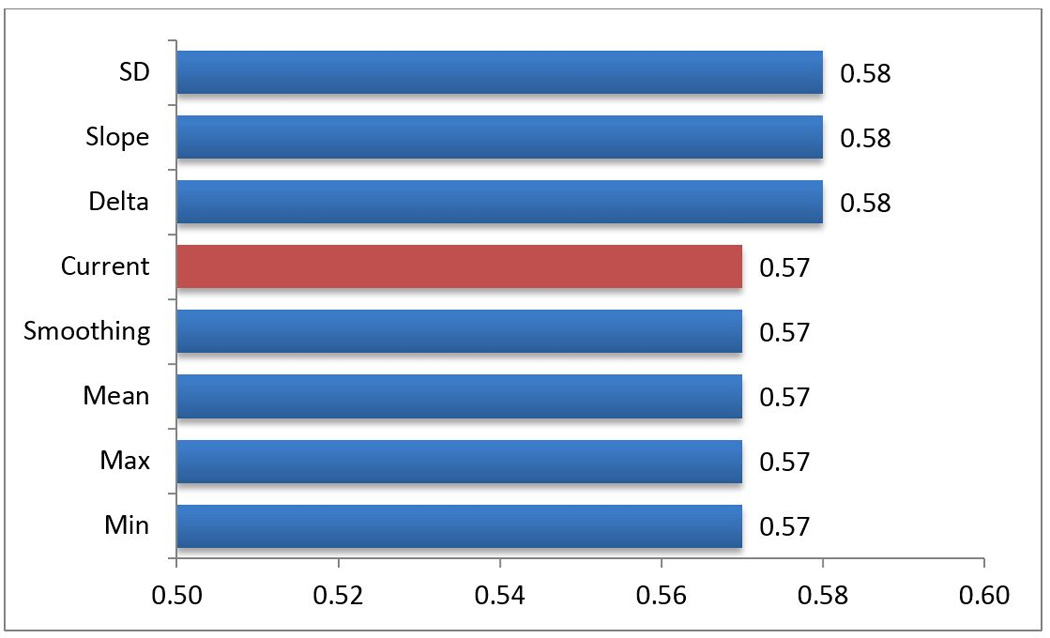
Results: A total of 269,999 patient admissions were included, which resulted in 16,452 outcomes. Overall, trends increased accuracy compared to a model containing only current vital signs (AUC 0.78 vs. 0.74; p<0.001). The methods that resulted in the greatest average increase in accuracy were the vital sign slope (AUC improvement 0.013) and minimum value (AUC improvement 0.012), while the change from the previous value resulted in an average worsening of the AUC (change in AUC -0.002). The AUC increased most for systolic blood pressure when trends were added (AUC improvement 0.05).
Conclusion: Vital sign trends increased the accuracy of models designed to detect critical illness on the wards. Our findings have important implications for clinicians at the bedside and for the development of early warning scores.
Keywords: Decision support techniques; Early diagnosis; Heart arrest; Hospital rapid response team; Physiologic monitoring; Vital signs.
Copyright © 2016 Elsevier Ireland Ltd. All rights reserved.
Figures
References
-
- Smith GB, Prytherch DR, Schmidt PE, Featherstone PI. Review and performance evaluation of aggregate weighted 'track and trigger' systems. Resuscitation. 2008;77:170–179. - PubMed
-
- Smith GB, Prytherch DR, Schmidt PE, Featherstone PI, Higgins B. A review, and performance evaluation, of single-parameter "track and trigger" systems. Resuscitation. 2008;79:11–21. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
