

Long-Term Efficacy, Tolerability, and Renal Safety of Atazanavir/Ritonavir-based Antiretroviral Therapy in a Cohort of Treatment-Naïve Patients with HIV-1 Infection: the REMAIN Study
- PMID: 26899539
- PMCID: PMC4975100
- DOI: 10.1080/15284336.2015.1112494
Long-Term Efficacy, Tolerability, and Renal Safety of Atazanavir/Ritonavir-based Antiretroviral Therapy in a Cohort of Treatment-Naïve Patients with HIV-1 Infection: the REMAIN Study
Abstract
Background: Boosted protease inhibitors (PIs), including ritonavir-boosted atazanavir (ATV/r), are a recommended option for the initial treatment of HIV-1 infection based upon clinical trial data; however, long-term real-life clinical data are limited.
Objective: We evaluated the long-term use of ATV/r as a component of antiretroviral combination therapy in the real-life setting in the REMAIN study.
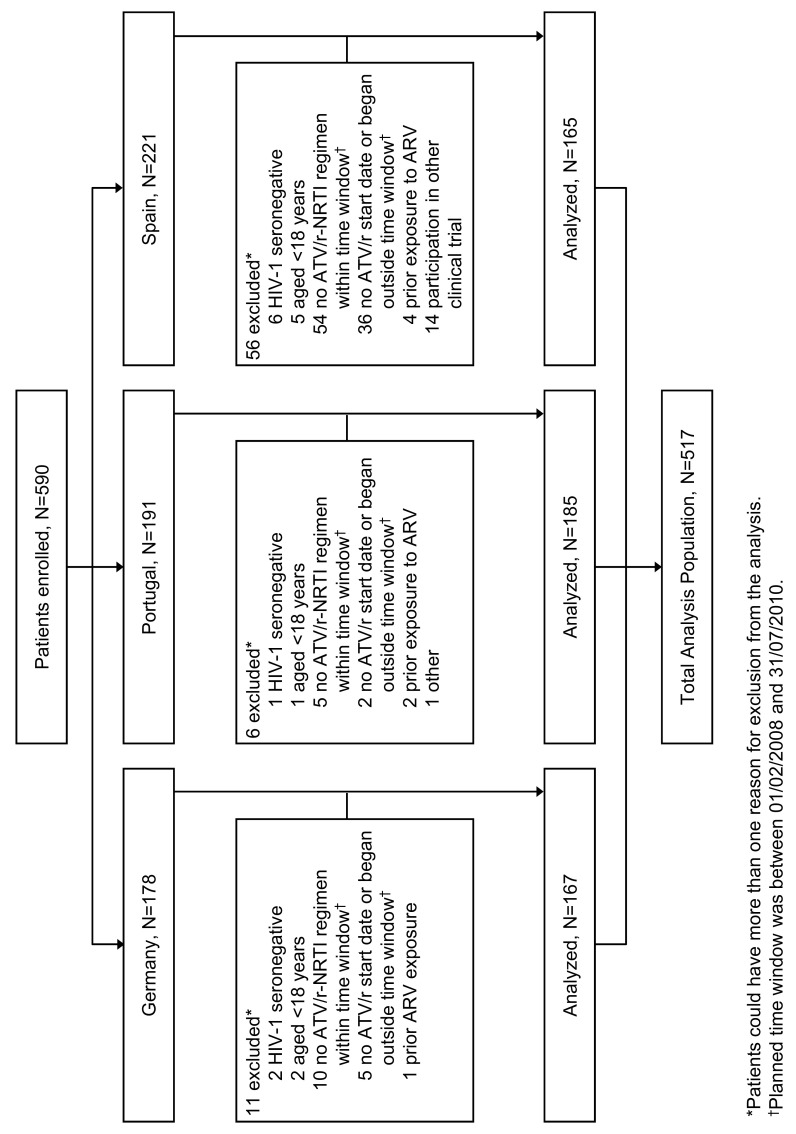
Methods: This was an observational cohort study conducted at sites across Germany, Portugal, and Spain. Retrospective historical and prospective longitudinal follow-up data were extracted every six months from medical records of HIV-infected treatment-naïve patients aged ≥ 18 years initiating a first-line ATV/r-containing regimen.
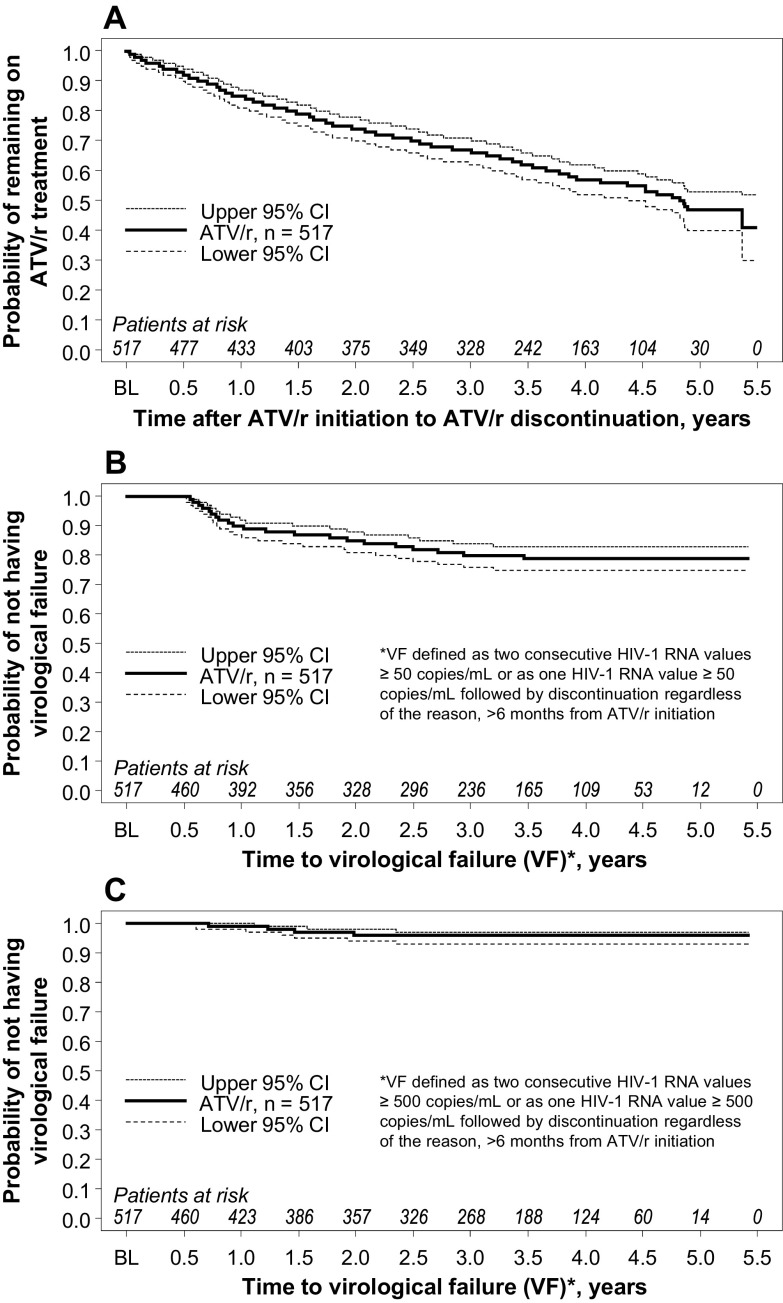
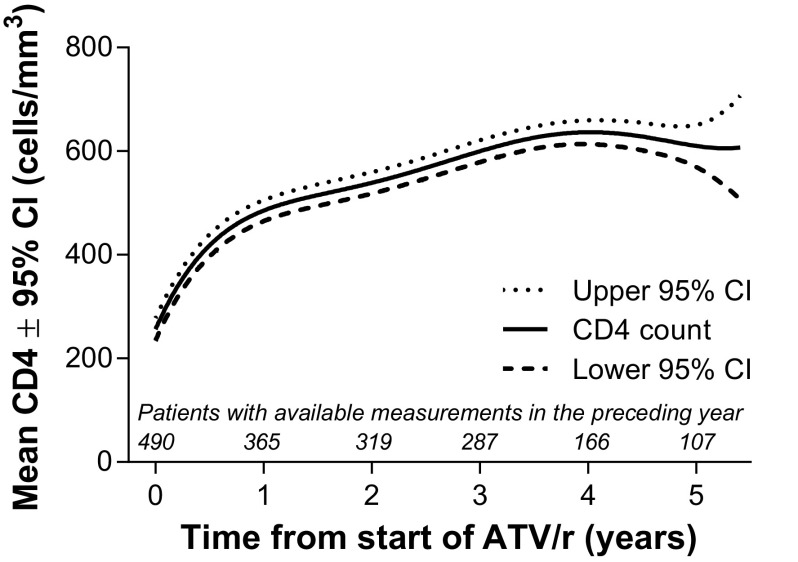
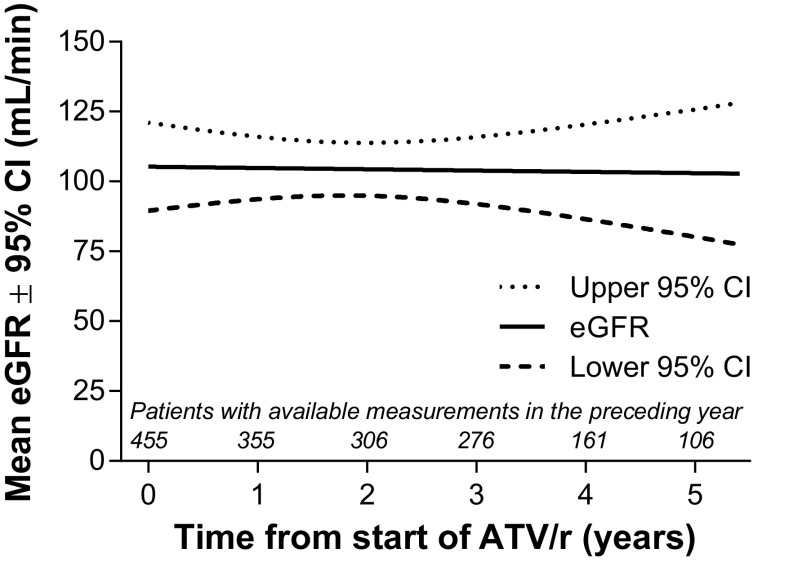
Results: Eligible patients (n = 517) were followed up for a median of 3.4 years. The proportion remaining on ATV/r at 5 years was 51.5% with an estimated Kaplan-Meier median time to treatment discontinuation of 4.9 years. Principal reasons for discontinuation were adverse events (15.9%; 8.9% due to hyperbilirubinemia) and virologic failure (6.8%). The Kaplan-Meier probability of not having virologic failure (HIV-1 RNA < 50 copies/mL) was 0.79 (95% CI: 0.75, 0.83) at five years. No treatment-emergent major PI resistance occurred. ATV/r was generally well tolerated during long-term treatment with no significant changes in estimated glomerular filtration rate over five years.
Conclusions: In a real-life clinical setting over five years, treatment-naïve patients with HIV-1 infection initiating an ATV/r-based regimen showed sustained virologic suppression, an overall treatment persistence rate of 51.5%, an absence of treatment-emergent major PI resistance mutations at virologic failure, a long-term safety profile consistent with that observed in clinical trials, and no significant decline in renal function.
Trial registration: ClinicalTrials.gov NCT01236235.
Keywords: HIV-1; antiretroviral therapy; estimated glomerular filtration rate; hyperbilirubinemia; observational study; persistence; resistance; ritonavir-boosted atazanavir.
Figures
References
-
- van Maarseveen N, Boucher C. Resistance to protease inhibitors. In: Geretti AM, editor. Antiretroviral resistance in clinical practice. London: 2006. - PubMed
-
- Department of Health and Human Services; 2014. [March 23, 2015]. Panel on antiretroviral guidelines for adults and adolescents. Guidelines for the use of antiretroviral agents in HIV-1-infected adults and adolescents.http://aidsinfo.nih.gov/contentfiles/AdultandAdolescentGL.pdf
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous