

Use of a Vaginal Ring Containing Dapivirine for HIV-1 Prevention in Women
- PMID: 26900902
- PMCID: PMC4993693
- DOI: 10.1056/NEJMoa1506110
Use of a Vaginal Ring Containing Dapivirine for HIV-1 Prevention in Women
Abstract
Background: Antiretroviral medications that are used as prophylaxis can prevent acquisition of human immunodeficiency virus type 1 (HIV-1) infection. However, in clinical trials among African women, the incidence of HIV-1 infection was not reduced, probably because of low adherence. Longer-acting methods of drug delivery, such as vaginal rings, may simplify use of antiretroviral medications and provide HIV-1 protection.
Methods: We conducted a phase 3, randomized, double-blind, placebo-controlled trial of a monthly vaginal ring containing dapivirine, a non-nucleoside HIV-1 reverse-transcriptase inhibitor, involving women between the ages of 18 and 45 years in Malawi, South Africa, Uganda, and Zimbabwe.
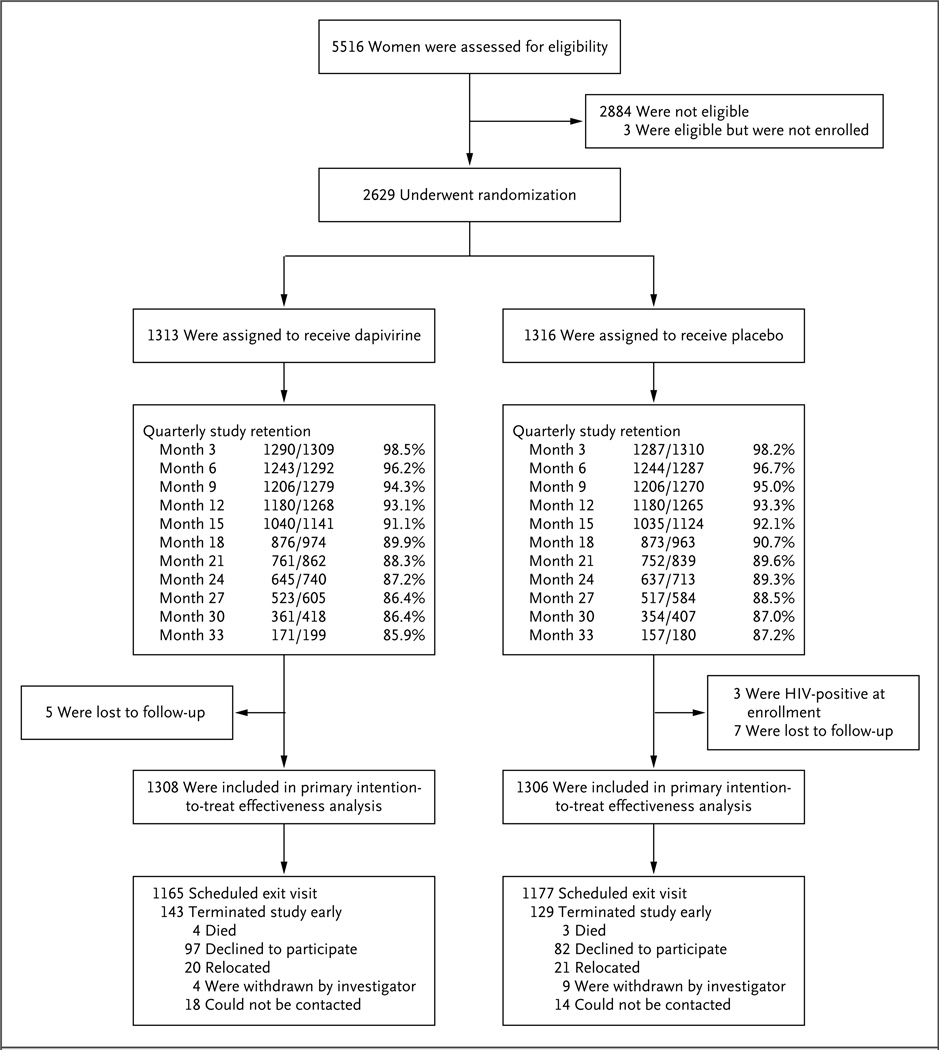
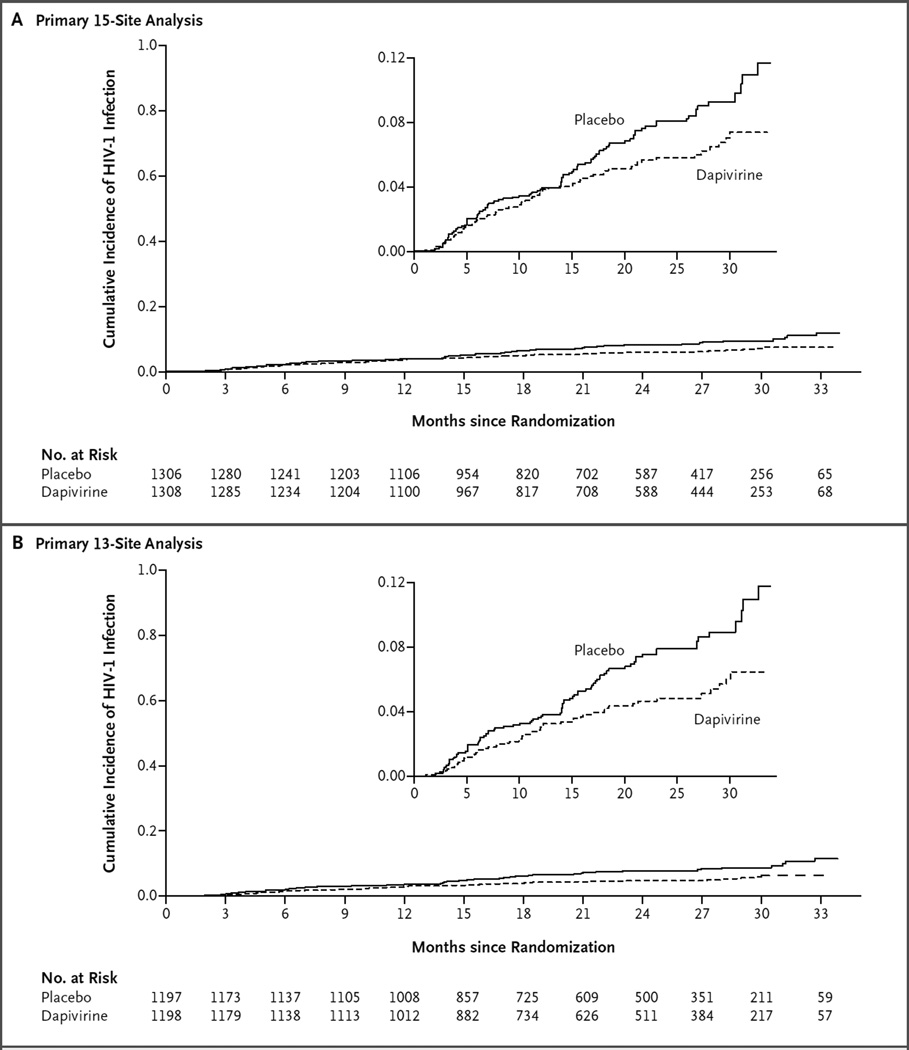
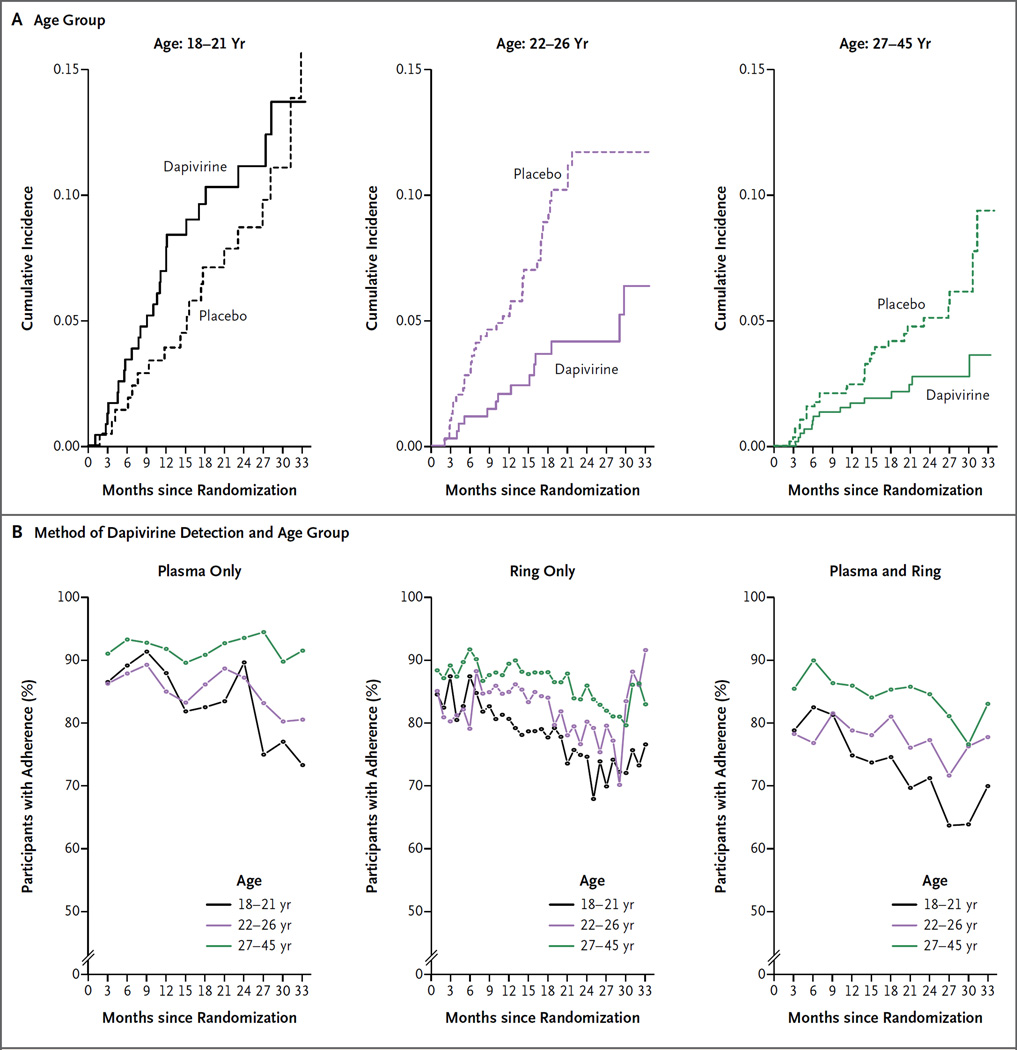
Results: Among the 2629 women who were enrolled, 168 HIV-1 infections occurred: 71 in the dapivirine group and 97 in the placebo group (incidence, 3.3 and 4.5 per 100 person-years, respectively). The incidence of HIV-1 infection in the dapivirine group was lower by 27% (95% confidence interval [CI], 1 to 46; P=0.046) than that in the placebo group. In an analysis that excluded data from two sites that had reduced rates of retention and adherence, the incidence of HIV-1 infection in the dapivirine group was lower by 37% (95% CI, 12 to 56; P=0.007) than that in the placebo group. In a post hoc analysis, higher rates of HIV-1 protection were observed among women over the age of 21 years (56%; 95% CI, 31 to 71; P<0.001) but not among those 21 years of age or younger (-27%; 95% CI, -133 to 31; P=0.45), a difference that was correlated with reduced adherence. The rates of adverse medical events and antiretroviral resistance among women who acquired HIV-1 infection were similar in the two groups.
Conclusions: A monthly vaginal ring containing dapivirine reduced the risk of HIV-1 infection among African women, with increased efficacy in subgroups with evidence of increased adherence. (Funded by the National Institutes of Health; ClinicalTrials.gov number, NCT01617096 .).
Figures
Comment in
-
Preventing HIV among Women - A Step Forward, but Much Farther to Go.N Engl J Med. 2016 Dec 1;375(22):2195-2196. doi: 10.1056/NEJMe1613661. N Engl J Med. 2016. PMID: 27959756 No abstract available.
-
Dapivirine Vaginal Ring for HIV-1 Prevention.N Engl J Med. 2017 Mar 9;376(10):995. doi: 10.1056/NEJMc1616546. N Engl J Med. 2017. PMID: 28273024 No abstract available.
-
Dapivirine Vaginal Ring for HIV-1 Prevention.N Engl J Med. 2017 Mar 9;376(10):994-5. doi: 10.1056/NEJMc1616546. N Engl J Med. 2017. PMID: 28276229 No abstract available.
References
-
- The Gap report. Geneva: Joint United Nations Programme on HIV/AIDS; 2014. ( http://www.unaids.org/sites/default/files/media_asset/UNAIDS_Gap_report_...)
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- UM1 AI069423/AI/NIAID NIH HHS/United States
- P30 MH062246/MH/NIMH NIH HHS/United States
- UM1 AI069519/AI/NIAID NIH HHS/United States
- UM1 AI068633/AI/NIAID NIH HHS/United States
- P30 AI094189/AI/NIAID NIH HHS/United States
- U01 AI068633/AI/NIAID NIH HHS/United States
- UM1 AI068615/AI/NIAID NIH HHS/United States
- UM1 AI106707/AI/NIAID NIH HHS/United States
- UM1 AI069469/AI/NIAID NIH HHS/United States
- UM1 AI069530/AI/NIAID NIH HHS/United States
- UM1 AI069518/AI/NIAID NIH HHS/United States
- UM1 AI069463/AI/NIAID NIH HHS/United States
- UM1 AI069422/AI/NIAID NIH HHS/United States
- UM1 AI069436/AI/NIAID NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical