

Association of Prenatal Diagnosis of Critical Congenital Heart Disease With Postnatal Brain Development and the Risk of Brain Injury
- PMID: 26902528
- PMCID: PMC5083633
- DOI: 10.1001/jamapediatrics.2015.4450
Association of Prenatal Diagnosis of Critical Congenital Heart Disease With Postnatal Brain Development and the Risk of Brain Injury
Abstract
Importance: The relationship of prenatal diagnosis of critical congenital heart disease (CHD) with brain injury and brain development is unknown. Given limited improvement of CHD outcomes with prenatal diagnosis, the effect of prenatal diagnosis on brain health may reveal additional benefits.
Objective: To compare the prevalence of preoperative and postoperative brain injury and the trajectory of brain development in neonates with prenatal vs postnatal diagnosis of CHD.
Design, setting, and participants: Cohort study of term newborns with critical CHD recruited consecutively from 2001 to 2013 at the University of California, San Francisco and the University of British Columbia. Term newborns with critical CHD were studied with brain magnetic resonance imaging preoperatively and postoperatively to determine brain injury severity and microstructural brain development with diffusion tensor imaging by measuring fractional anisotropy and the apparent diffusion coefficient. Comparisons of magnetic resonance imaging findings and clinical variables were made between prenatal and postnatal diagnosis of critical CHD. A total of 153 patients with transposition of the great arteries and single ventricle physiology were included in this analysis.
Main outcomes and measures: The presence of brain injury on the preoperative brain magnetic resonance imaging and the trajectory of postnatal brain microstructural development.
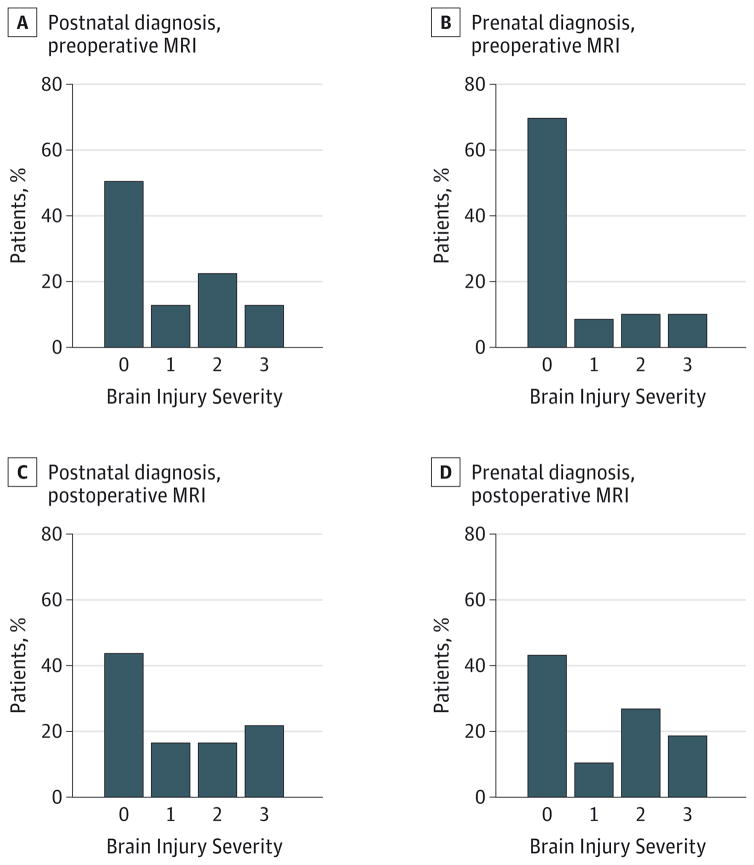
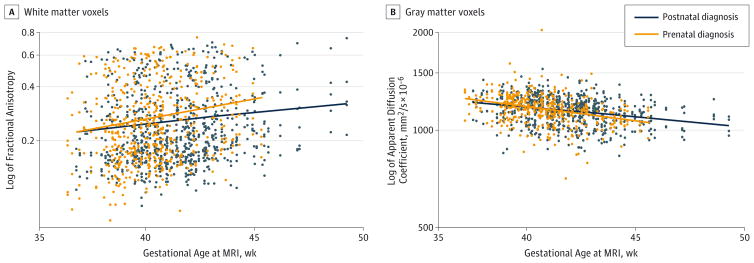
Results: Among 153 patients (67% male), 96 had transposition of the great arteries and 57 had single ventricle physiology. The presence of brain injury was significantly higher in patients with postnatal diagnosis of critical CHD (41 of 86 [48%]) than in those with prenatal diagnosis (16 of 67 [24%]) (P = .003). Patients with prenatal diagnosis demonstrated faster brain development in white matter fractional anisotropy (rate of increase, 2.2%; 95% CI, 0.1%-4.2%; P = .04) and gray matter apparent diffusion coefficient (rate of decrease, 0.6%; 95% CI, 0.1%-1.2%; P = .02). Patients with prenatal diagnosis had lower birth weight (mean, 3184.5 g; 95% CI, 3050.3-3318.6) than those with postnatal diagnosis (mean, 3397.6 g; 95% CI, 3277.6-3517.6) (P = .02). Those with prenatal diagnosis had an earlier estimated gestational age at delivery (mean, 38.6 weeks; 95% CI, 38.2-38.9) than those with postnatal diagnosis (mean, 39.1 weeks; 95% CI, 38.8-39.5) (P = .03).
Conclusions and relevance: Newborns with prenatal diagnosis of single ventricle physiology and transposition of the great arteries demonstrate less preoperative brain injury and more robust microstructural brain development than those with postnatal diagnosis. These results are likely secondary to improved cardiovascular stability. The impact of these findings on neurodevelopmental outcomes warrants further study.
Conflict of interest statement
Disclosures: None reported.
Figures
References
-
- American Institute of Ultrasound in Medicine. AIUM practice guideline for the performance of fetal echocardiography. J Ultrasound Med. 2013;32(6):1067–1082. - PubMed
-
- Carvalho JS, Allan LD, Chaoui R, et al. International Society of Ultrasound in Obstetrics and Gynecology. ISUOG practice guidelines (updated): sonographic screening examination of the fetal heart. Ultrasound Obstet Gynecol. 2013;41(3):348–359. - PubMed
-
- Tometzki AJ, Suda K, Kohl T, Kovalchin JP, Silverman NH. Accuracy of prenatal echocardiographic diagnosis and prognosis of fetuses with conotruncal anomalies. J Am Coll Cardiol. 1999;33(6):1696–1701. - PubMed
-
- Allan LD, Sharland GK, Milburn A, et al. Prospective diagnosis of 1,006 consecutive cases of congenital heart disease in the fetus. J Am Coll Cardiol. 1994;23(6):1452–1458. - PubMed
-
- Donofrio MT, Moon-Grady AJ, Hornberger LK, et al. American Heart Association Adults With Congenital Heart Disease Joint Committee of the Council on Cardiovascular Disease in the Young and Council on Clinical Cardiology, Council on Cardiovascular Surgery and Anesthesia, and Council on Cardiovascular and Stroke Nursing. Diagnosis and treatment of fetal cardiac disease: a scientific statement from the American Heart Association. Circulation. 2014;129(21):2183–2242. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
