

Risk of recurrence of Barrett's esophagus after successful endoscopic therapy
- PMID: 26902843
- PMCID: PMC4937826
- DOI: 10.1016/j.gie.2016.02.009
Risk of recurrence of Barrett's esophagus after successful endoscopic therapy
Abstract
Background and aims: Previous estimates of incidence of intestinal metaplasia (IM) recurrence after achieving complete remission of IM (CRIM) through endoscopic therapy of Barrett's esophagus (BE) have varied widely. We performed a systematic review and meta-analysis of studies to estimate an accurate recurrence risk after CRIM.
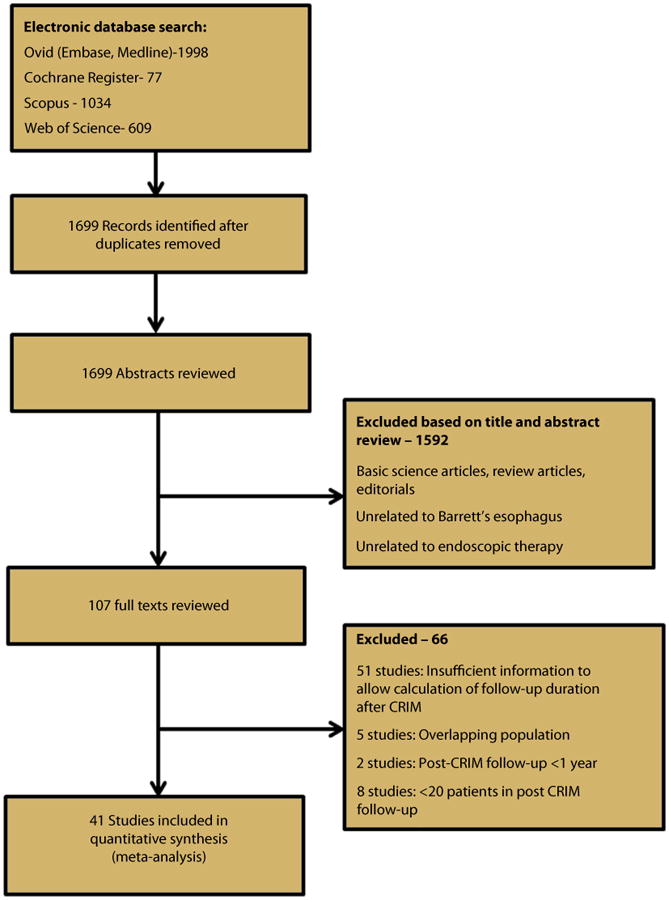
Methods: We performed a systematic search of multiple literature databases through June 2015 to identify studies reporting long-term follow-up after achieving CRIM through endoscopic therapy. Pooled incidence rate (IR) of recurrent IM, dysplastic BE, and high-grade dysplasia (HGD)/esophageal adenocarcinoma (EAC) per person-year of follow-up after CRIM was estimated. Factors associated with recurrence were also assessed.
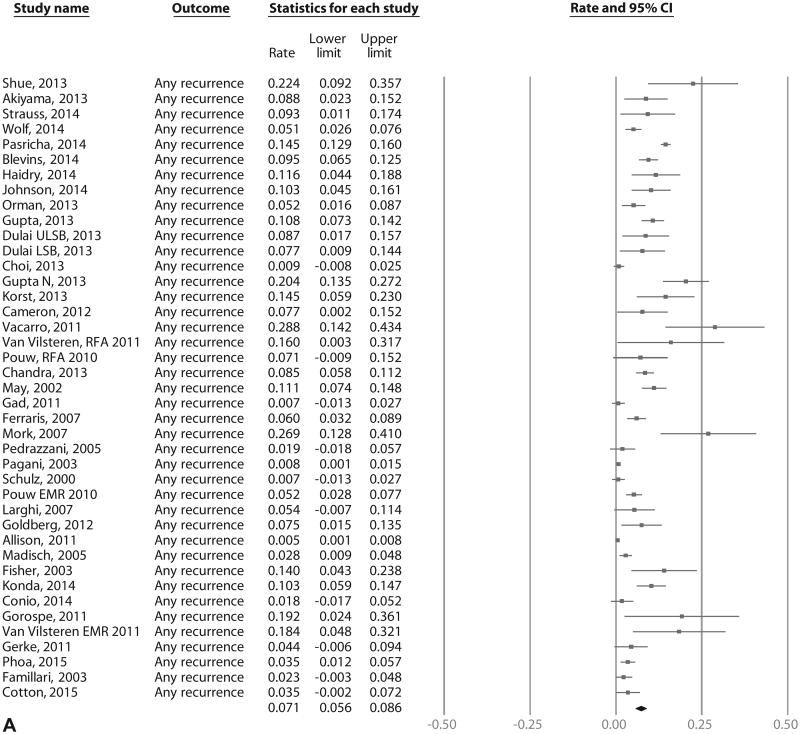
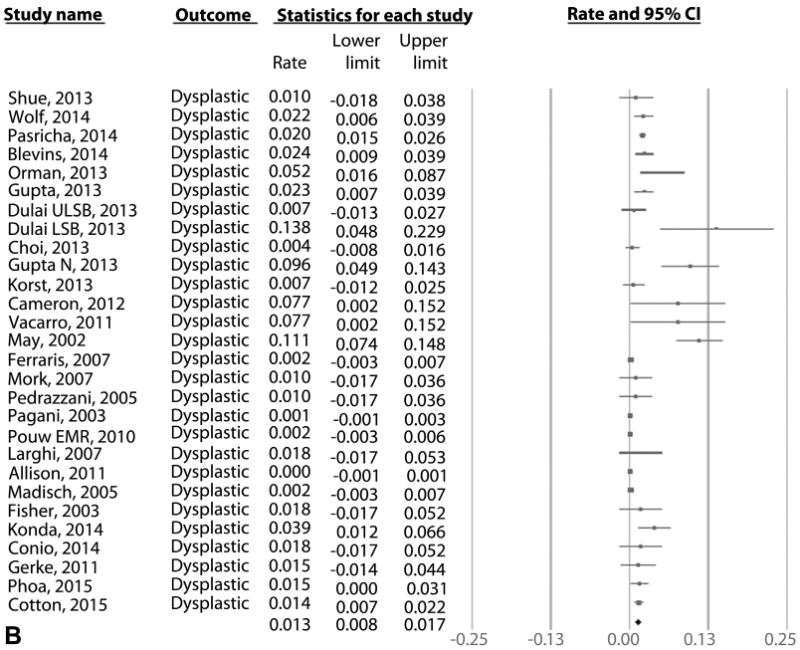
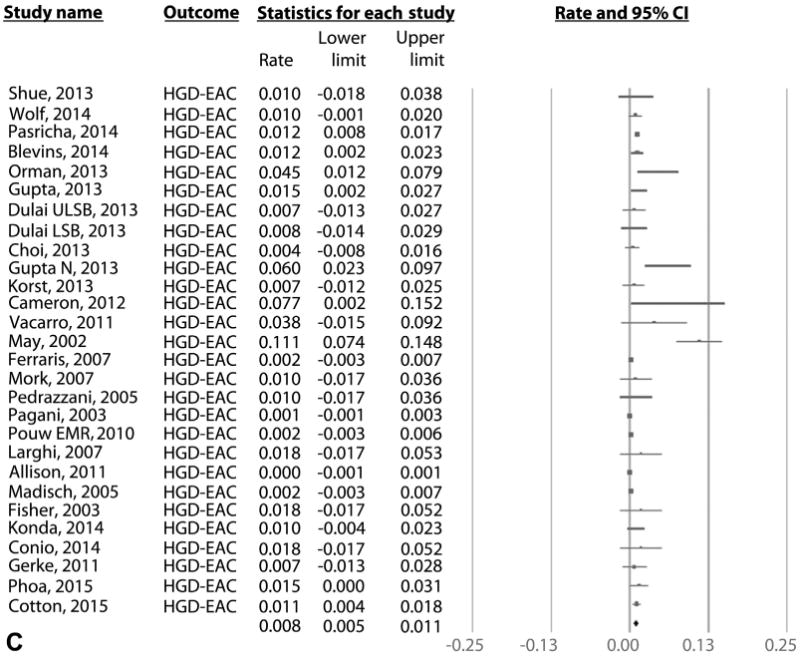
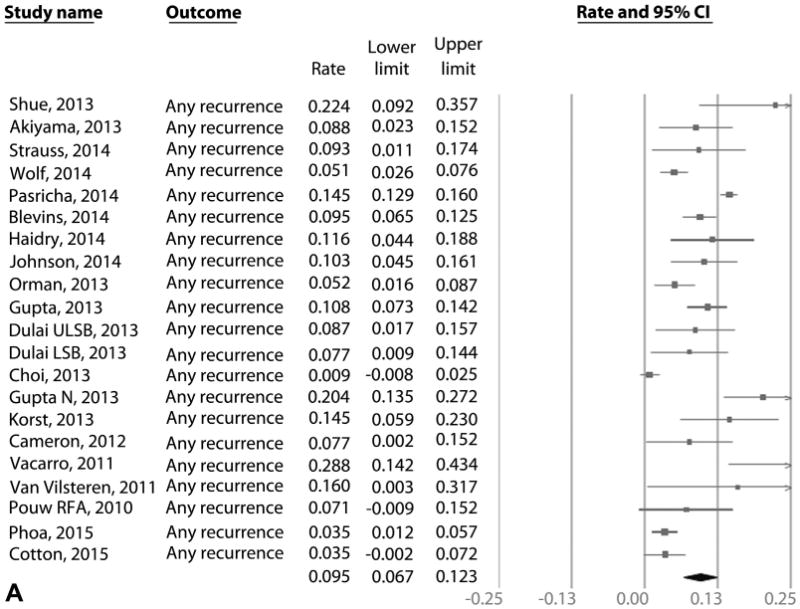
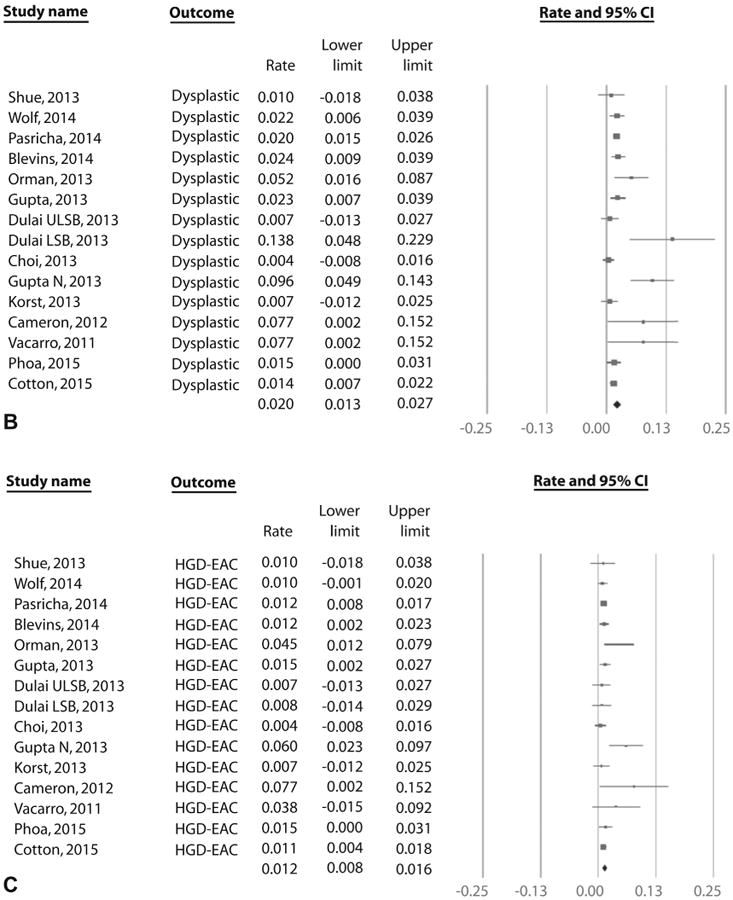
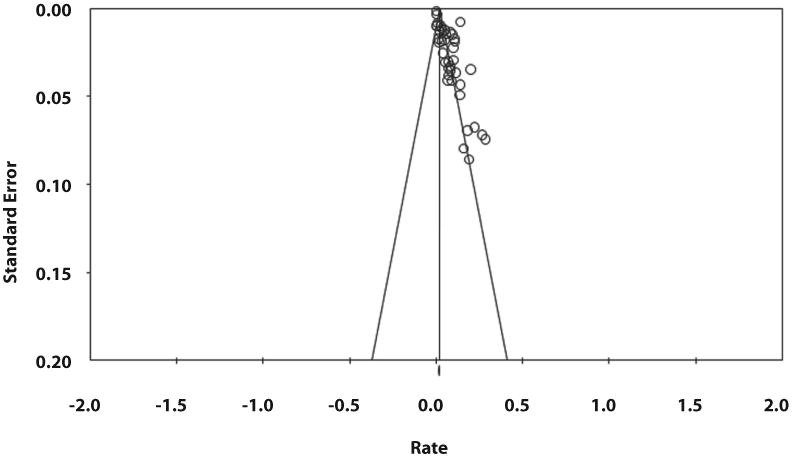
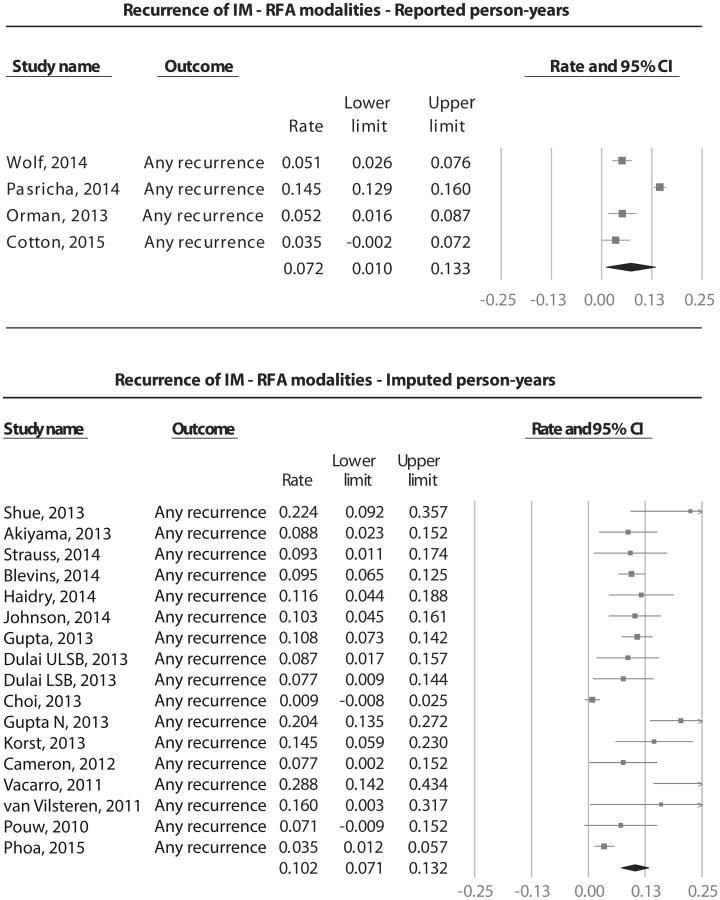
Results: We identified 41 studies that reported 795 cases of recurrence in 4443 patients over 10,427 patient-years of follow-up. This included 21 radiofrequency ablation studies that reported 603 cases of IM recurrence in 3186 patients over 5741 patient-years of follow-up. Pooled IRs of recurrent IM, dysplastic BE, and HGD/EAC after radiofrequency ablation were 9.5% (95% CI, 6.7-12.3), 2.0% (95% CI, 1.3-2.7), and 1.2% (95% CI, .8-1.6) per patient-year, respectively. When all endoscopic modalities were included, pooled IRs of recurrent IM, dysplastic BE, and HGD/EAC were 7.1% (95% CI, 5.6-8.6), 1.3% (95% CI, .8-1.7), and .8% (95% CI, .5-1.1) per patient-year, respectively. Substantial heterogeneity was noted. Increasing age and BE length were predictive of recurrence; 97% of recurrences were treated endoscopically.
Conclusions: The incidence of recurrence after achieving CRIM through endoscopic therapy was substantial. A small minority of recurrences were dysplastic BE and HGD/EAC. Hence, continued surveillance after CRIM is imperative. Additional studies with long-term follow-up are needed.
Copyright © 2016 American Society for Gastrointestinal Endoscopy. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Evans JA, Early DS, Fukami N, et al. The role of endoscopy in Barrett's esophagus and other premalignant conditions of the esophagus. Gastrointest Endosc. 2012;76:1087–94. - PubMed
-
- Blevins CH, Iyer PG. Endoscopic therapy for Barrett's oesophagus. Best Pract Res Clin Gastroenterol. 2015;29:167–77. - PubMed
-
- Shaheen NJ, Sharma P, Overholt BF, et al. Radiofrequency ablation in Barrett's esophagus with dysplasia. N Engl J Med. 2009;360:2277–88. - PubMed
-
- Phoa KN, van Vilsteren FG, Weusten BL, et al. Radiofrequency ablation vs endoscopic surveillance for patients with Barrett esophagus and low-grade dysplasia: a randomized clinical trial. JAMA. 2014;311:1209–17. - PubMed
Publication types
MeSH terms
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
