

Assessment of Clinical Criteria for Sepsis: For the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3)
- PMID: 26903335
- PMCID: PMC5433435
- DOI: 10.1001/jama.2016.0288
Assessment of Clinical Criteria for Sepsis: For the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3)
Erratum in
-
Incorrect Data.JAMA. 2016 May 24-31;315(20):2237. doi: 10.1001/jama.2016.5850. JAMA. 2016. PMID: 27218643 No abstract available.
Abstract
Importance: The Third International Consensus Definitions Task Force defined sepsis as "life-threatening organ dysfunction due to a dysregulated host response to infection." The performance of clinical criteria for this sepsis definition is unknown.
Objective: To evaluate the validity of clinical criteria to identify patients with suspected infection who are at risk of sepsis.
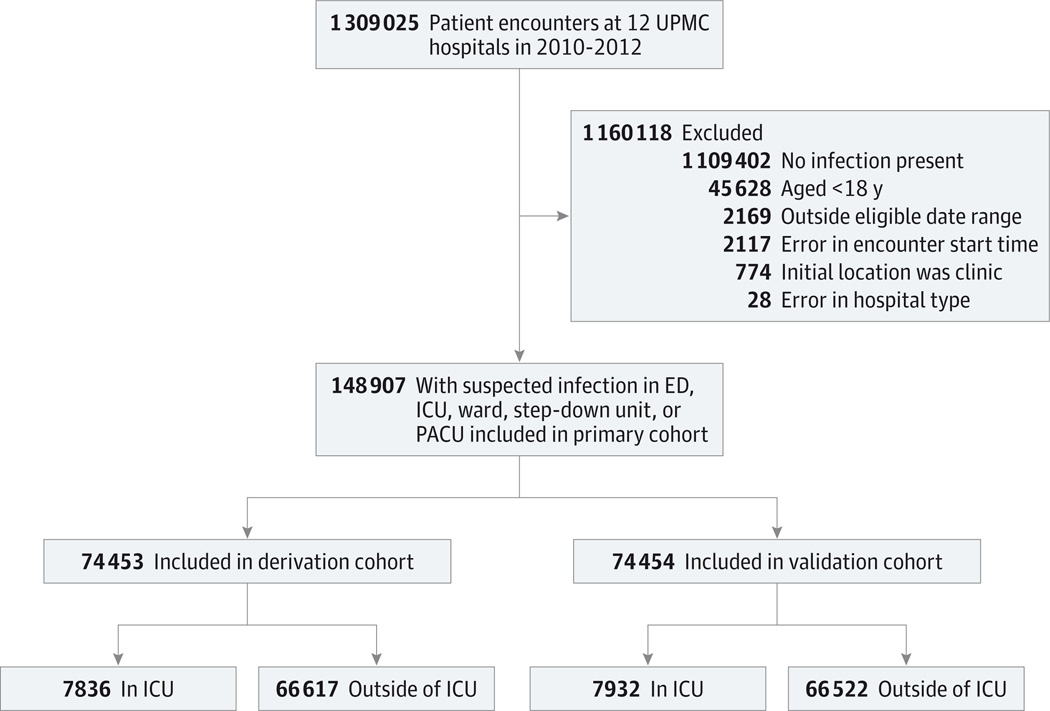
Design, settings, and population: Among 1.3 million electronic health record encounters from January 1, 2010, to December 31, 2012, at 12 hospitals in southwestern Pennsylvania, we identified those with suspected infection in whom to compare criteria. Confirmatory analyses were performed in 4 data sets of 706,399 out-of-hospital and hospital encounters at 165 US and non-US hospitals ranging from January 1, 2008, until December 31, 2013.
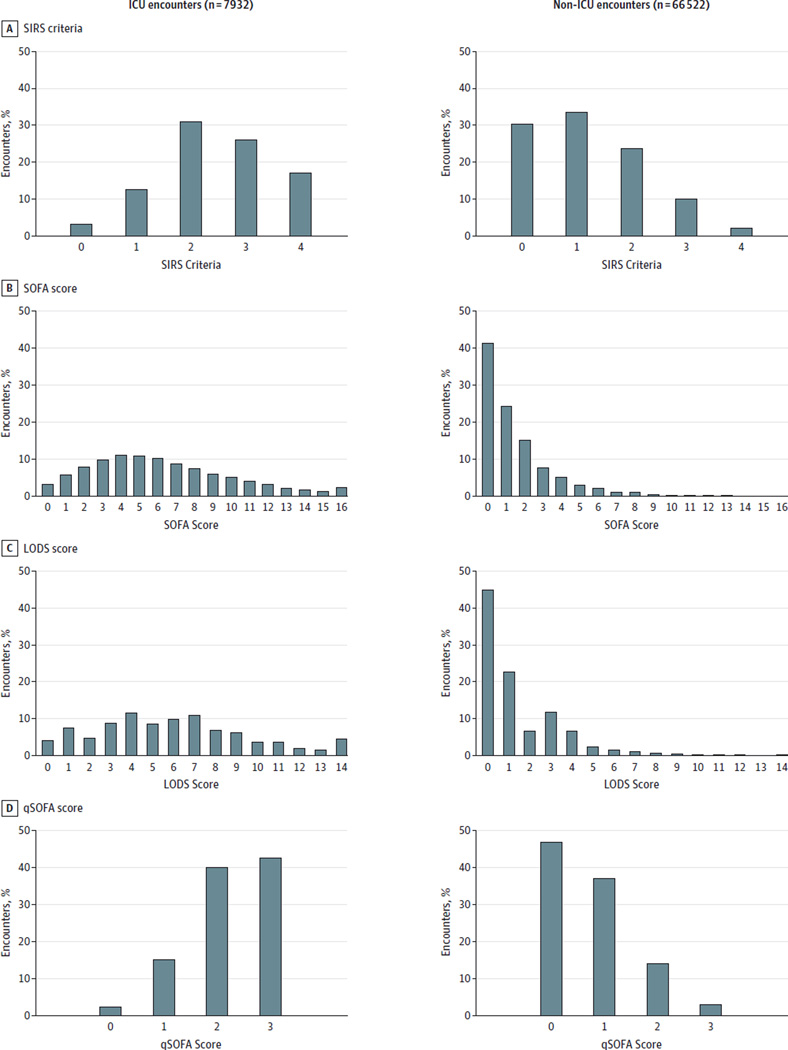
Exposures: Sequential [Sepsis-related] Organ Failure Assessment (SOFA) score, systemic inflammatory response syndrome (SIRS) criteria, Logistic Organ Dysfunction System (LODS) score, and a new model derived using multivariable logistic regression in a split sample, the quick Sequential [Sepsis-related] Organ Failure Assessment (qSOFA) score (range, 0-3 points, with 1 point each for systolic hypotension [≤100 mm Hg], tachypnea [≥22/min], or altered mentation).
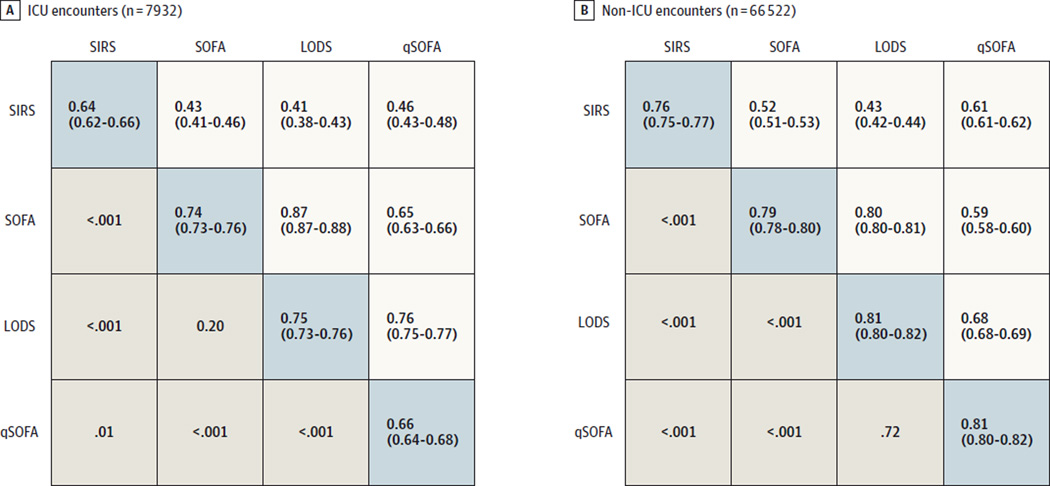
Main outcomes and measures: For construct validity, pairwise agreement was assessed. For predictive validity, the discrimination for outcomes (primary: in-hospital mortality; secondary: in-hospital mortality or intensive care unit [ICU] length of stay ≥3 days) more common in sepsis than uncomplicated infection was determined. Results were expressed as the fold change in outcome over deciles of baseline risk of death and area under the receiver operating characteristic curve (AUROC).
Results: In the primary cohort, 148,907 encounters had suspected infection (n = 74,453 derivation; n = 74,454 validation), of whom 6347 (4%) died. Among ICU encounters in the validation cohort (n = 7932 with suspected infection, of whom 1289 [16%] died), the predictive validity for in-hospital mortality was lower for SIRS (AUROC = 0.64; 95% CI, 0.62-0.66) and qSOFA (AUROC = 0.66; 95% CI, 0.64-0.68) vs SOFA (AUROC = 0.74; 95% CI, 0.73-0.76; P < .001 for both) or LODS (AUROC = 0.75; 95% CI, 0.73-0.76; P < .001 for both). Among non-ICU encounters in the validation cohort (n = 66 522 with suspected infection, of whom 1886 [3%] died), qSOFA had predictive validity (AUROC = 0.81; 95% CI, 0.80-0.82) that was greater than SOFA (AUROC = 0.79; 95% CI, 0.78-0.80; P < .001) and SIRS (AUROC = 0.76; 95% CI, 0.75-0.77; P < .001). Relative to qSOFA scores lower than 2, encounters with qSOFA scores of 2 or higher had a 3- to 14-fold increase in hospital mortality across baseline risk deciles. Findings were similar in external data sets and for the secondary outcome.
Conclusions and relevance: Among ICU encounters with suspected infection, the predictive validity for in-hospital mortality of SOFA was not significantly different than the more complex LODS but was statistically greater than SIRS and qSOFA, supporting its use in clinical criteria for sepsis. Among encounters with suspected infection outside of the ICU, the predictive validity for in-hospital mortality of qSOFA was statistically greater than SOFA and SIRS, supporting its use as a prompt to consider possible sepsis.
Conflict of interest statement
Figures

Comment in
-
Clinical Criteria to Identify Patients With Sepsis.JAMA. 2016 Jul 26;316(4):453. doi: 10.1001/jama.2016.6407. JAMA. 2016. PMID: 27458952 Free PMC article. No abstract available.
-
Clinical Criteria to Identify Patients With Sepsis.JAMA. 2016 Jul 26;316(4):453-4. doi: 10.1001/jama.2016.6410. JAMA. 2016. PMID: 27458953 No abstract available.
-
Clinical Criteria to Identify Patients With Sepsis--Reply.JAMA. 2016 Jul 26;316(4):454. doi: 10.1001/jama.2016.6413. JAMA. 2016. PMID: 27458955 No abstract available.
-
Logistic Regression: Relating Patient Characteristics to Outcomes.JAMA. 2016 Aug 2;316(5):533-4. doi: 10.1001/jama.2016.7653. JAMA. 2016. PMID: 27483067 No abstract available.
-
Assessment of clinical criteria for sepsis-was the cart put before the horse?J Thorac Dis. 2016 Aug;8(8):E816-8. doi: 10.21037/jtd.2016.07.51. J Thorac Dis. 2016. PMID: 27618927 Free PMC article. No abstract available.
-
Quick sequential organ failure assessment: big databases vs. intelligent doctors.J Thorac Dis. 2016 Sep;8(9):E996-E998. doi: 10.21037/jtd.2016.07.78. J Thorac Dis. 2016. PMID: 27747044 Free PMC article. No abstract available.
-
qSOFA for Identifying Sepsis Among Patients With Infection.JAMA. 2017 Jan 17;317(3):267-268. doi: 10.1001/jama.2016.19684. JAMA. 2017. PMID: 28114531 No abstract available.
-
[Intensive care studies from 2016/2017].Anaesthesist. 2017 Sep;66(9):690-713. doi: 10.1007/s00101-017-0339-8. Anaesthesist. 2017. PMID: 28667421 Free PMC article. German. No abstract available.
-
qSOFA, Cue Confusion.Ann Intern Med. 2018 Feb 20;168(4):293-295. doi: 10.7326/M17-3415. Epub 2018 Feb 6. Ann Intern Med. 2018. PMID: 29404580 No abstract available.
References
-
- Liu V, Escobar GJ, Greene JD, et al. Hospital deaths in patients with sepsis from 2 independent cohorts. JAMA. 2014;312(1):90–92. - PubMed
-
- Angus DC, Linde-Zwirble WT, Lidicker J, Clermont G, Carcillo J, Pinsky MR. Epidemiology of severe sepsis in the United States: analysis of incidence, outcome, and associated costs of care. Crit Care Med. 2001;29(7):1303–1310. - PubMed
-
- Levy MM, Fink MP, Marshall JC, et al. SCCM/ESICM/ACCP/ATS/SIS. 2001 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference. Crit Care Med. 2003;31(4):1250–1256. - PubMed
-
- Bone RC, Balk RA, Cerra FB, et al. ACCP/SCCM Consensus Conference Committee; American College of Chest Physicians/Society of Critical Care Medicine. Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. Chest. 1992;101(6):1644–1655. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
