

Prevention of cardiac dysfunction during adjuvant breast cancer therapy (PRADA): a 2 × 2 factorial, randomized, placebo-controlled, double-blind clinical trial of candesartan and metoprolol
- PMID: 26903532
- PMCID: PMC4887703
- DOI: 10.1093/eurheartj/ehw022
Prevention of cardiac dysfunction during adjuvant breast cancer therapy (PRADA): a 2 × 2 factorial, randomized, placebo-controlled, double-blind clinical trial of candesartan and metoprolol
Abstract
Aims: Contemporary adjuvant treatment for early breast cancer is associated with improved survival but at the cost of increased risk of cardiotoxicity and cardiac dysfunction. We tested the hypothesis that concomitant therapy with the angiotensin receptor blocker candesartan or the β-blocker metoprolol will alleviate the decline in left ventricular ejection fraction (LVEF) associated with adjuvant, anthracycline-containing regimens with or without trastuzumab and radiation.
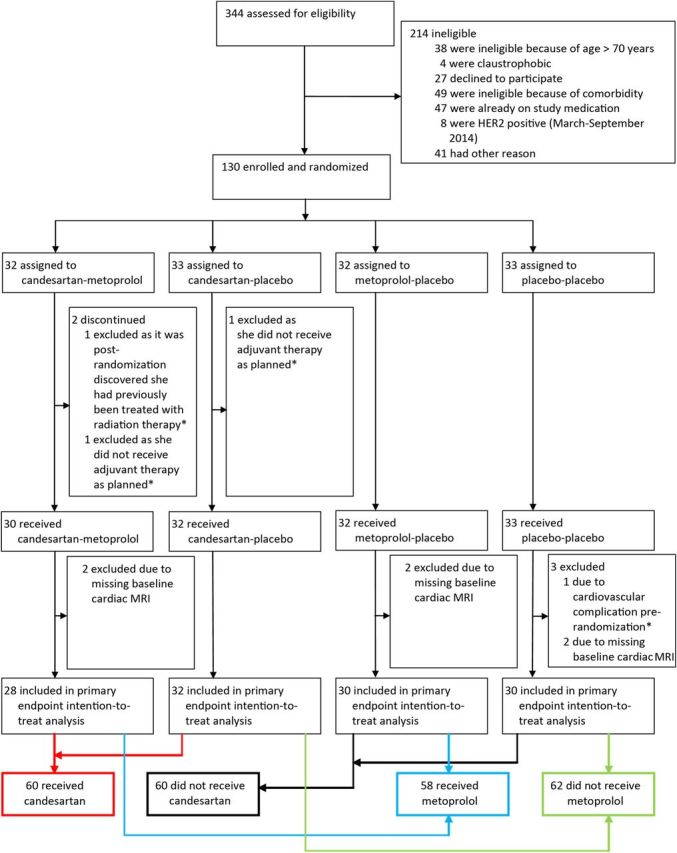
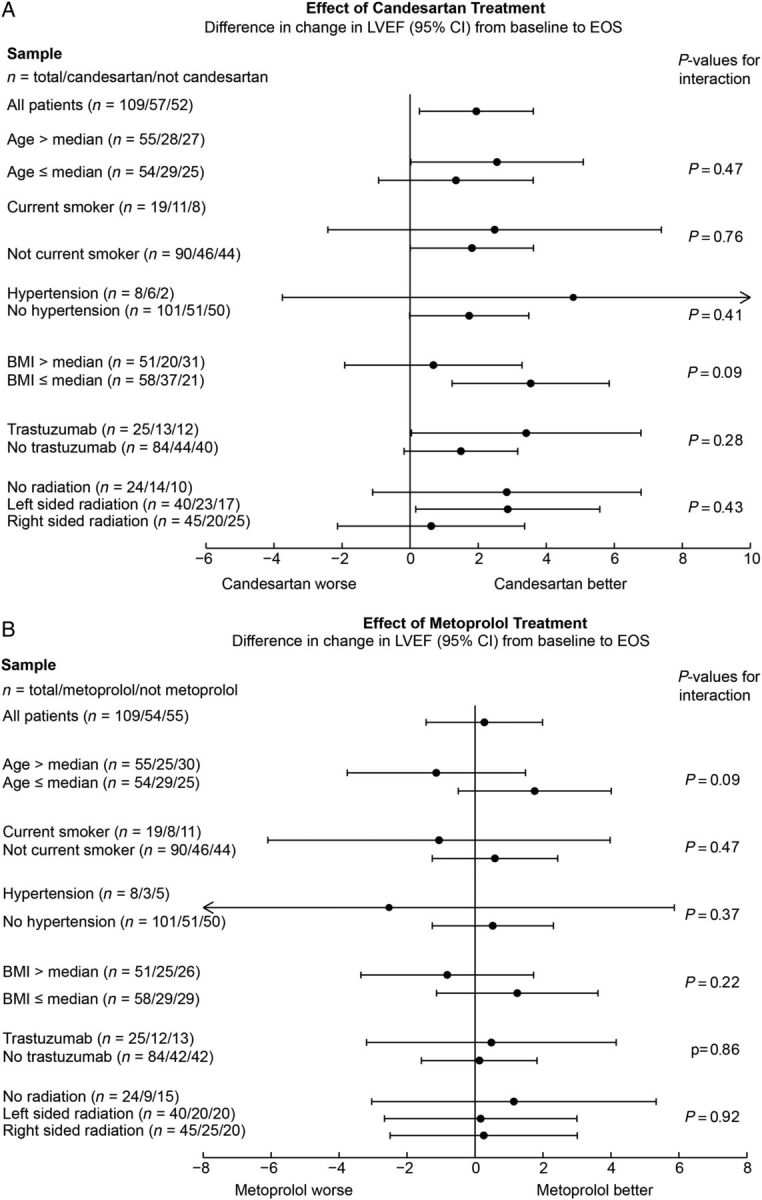
Methods and results: In a 2 × 2 factorial, randomized, placebo-controlled, double-blind trial, we assigned 130 adult women with early breast cancer and no serious co-morbidity to the angiotensin receptor blocker candesartan cilexetil, the β-blocker metoprolol succinate, or matching placebos in parallel with adjuvant anticancer therapy. The primary outcome measure was change in LVEF by cardiac magnetic resonance imaging. A priori, a change of 5 percentage points was considered clinically important. There was no interaction between candesartan and metoprolol treatments (P = 0.530). The overall decline in LVEF was 2.6 (95% CI 1.5, 3.8) percentage points in the placebo group and 0.8 (95% CI -0.4, 1.9) in the candesartan group in the intention-to-treat analysis (P-value for between-group difference: 0.026). No effect of metoprolol on the overall decline in LVEF was observed.
Conclusion: In patients treated for early breast cancer with adjuvant anthracycline-containing regimens with or without trastuzumab and radiation, concomitant treatment with candesartan provides protection against early decline in global left ventricular function.
Keywords: Angiotensin antagonist; Biomarkers; Breast cancer; Cardiomyopathy; Imaging; β-Blocker.
© The Author 2016. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures
Comment in
-
Cardioprotection: Cardiotoxicity of anticancer therapy.Nat Rev Cardiol. 2016 Apr;13(4):183. doi: 10.1038/nrcardio.2016.39. Epub 2016 Mar 10. Nat Rev Cardiol. 2016. PMID: 26961065 No abstract available.
-
Cardiotoxicity of breast cancer treatment: no easy solution for an important long-term problem.Eur Heart J. 2016 Jun 1;37(21):1681-3. doi: 10.1093/eurheartj/ehw133. Epub 2016 Apr 7. Eur Heart J. 2016. PMID: 27055813 No abstract available.
References
-
- Ewer MS, Ewer SM. Cardiotoxicity of anticancer treatments. Nat Rev Cardiol 2015;12:547–558. - PubMed
-
- Drafts BC, Twomley KM, D'Agostino R, Lawrence J, Avis N, Ellis LR, Thohan V, Jordan J, Melin SA, Torti FM, Little WC, Hamilton CA, Hundley WG. Low to moderate dose anthracycline-based chemotherapy is associated with early noninvasive imaging evidence of subclinical cardiovascular disease. JACC Cardiovasc Imaging 2013;6:877–885. - PMC - PubMed
-
- Chien KR. Herceptin and the heart—a molecular modifier of cardiac failure. N Engl J Med 2006;354:789–790. - PubMed
-
- Tan TC, Neilan TG, Francis S, Plana JC, Scherrer-Crosbie M. Anthracycline-induced cardiomyopathy in adults. Compr Physiol 2015;5:1517–1540. - PubMed
-
- Vejpongsa P, Yeh ET. Prevention of anthracycline-induced cardiotoxicity: challenges and opportunities. J Am Coll Cardiol 2014;64:938–945. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
