

Trial Design and Objectives for Castration-Resistant Prostate Cancer: Updated Recommendations From the Prostate Cancer Clinical Trials Working Group 3
- PMID: 26903579
- PMCID: PMC4872347
- DOI: 10.1200/JCO.2015.64.2702
Trial Design and Objectives for Castration-Resistant Prostate Cancer: Updated Recommendations From the Prostate Cancer Clinical Trials Working Group 3
Abstract
Purpose: Evolving treatments, disease phenotypes, and biology, together with a changing drug development environment, have created the need to revise castration-resistant prostate cancer (CRPC) clinical trial recommendations to succeed those from prior Prostate Cancer Clinical Trials Working Groups.
Methods: An international expert committee of prostate cancer clinical investigators (the Prostate Cancer Clinical Trials Working Group 3 [PCWG3]) was reconvened and expanded and met in 2012-2015 to formulate updated criteria on the basis of emerging trial data and validation studies of the Prostate Cancer Clinical Trials Working Group 2 recommendations.
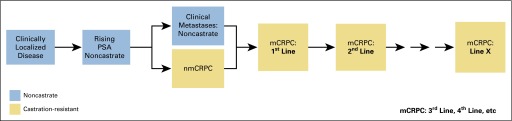
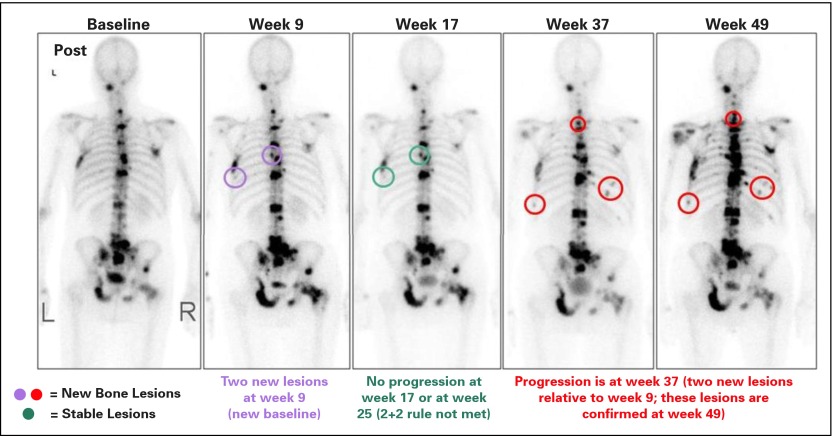
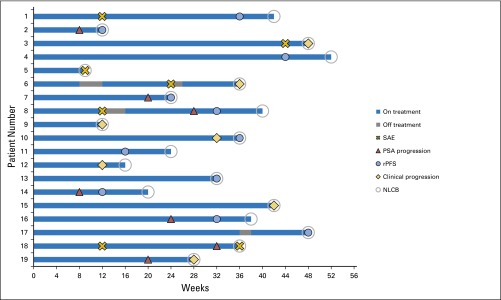
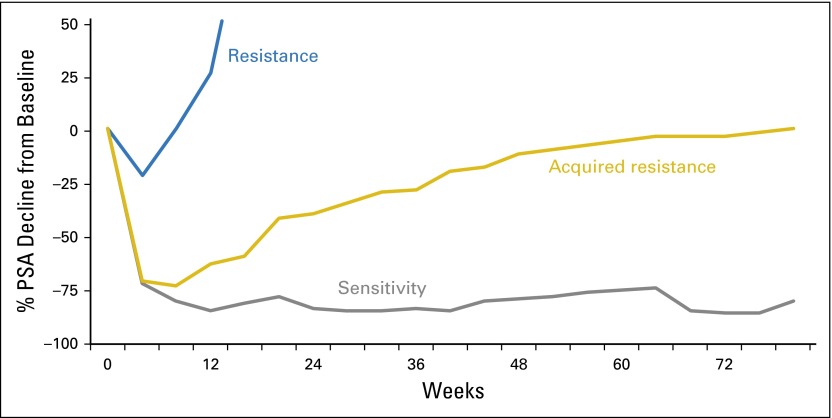
Results: PCWG3 recommends that baseline patient assessment include tumor histology, detailed records of prior systemic treatments and responses, and a detailed reporting of disease subtypes based on an anatomic pattern of metastatic spread. New recommendations for trial outcome measures include the time to event end point of symptomatic skeletal events, as well as time to first metastasis and time to progression for trials in the nonmetastatic CRPC state. PCWG3 introduces the concept of no longer clinically benefiting to underscore the distinction between first evidence of progression and the clinical need to terminate or change treatment, and the importance of documenting progression in existing lesions as distinct from the development of new lesions. Serial biologic profiling using tumor samples from biopsies, blood-based diagnostics, and/or imaging is also recommended to gain insight into mechanisms of resistance and to identify predictive biomarkers of sensitivity for use in prospective trials.
Conclusion: PCWG3 moves drug development closer to unmet needs in clinical practice by focusing on disease manifestations most likely to affect prognosis adversely for therapeutics tested in both nonmetastatic and metastatic CRPC populations. Consultation with regulatory authorities is recommended if a trial is intended to seek support for drug approval.
© 2016 by American Society of Clinical Oncology.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest are found in the article online at
Figures
References
-
- Bubley GJ, Carducci M, Dahut W, et al. Eligibility and response guidelines for phase II clinical trials in androgen-independent prostate cancer: Recommendations from the Prostate-Specific Antigen Working Group. J Clin Oncol. 1999;17:3461–3467. - PubMed
-
- Tannock IF, de Wit R, Berry WR, et al. TAX 327 Investigators Docetaxel plus prednisone or mitoxantrone plus prednisone for advanced prostate cancer. N Engl J Med. 2004;351:1502–1512. - PubMed
-
- Petrylak DP, Tangen CM, Hussain MH, et al. Docetaxel and estramustine compared with mitoxantrone and prednisone for advanced refractory prostate cancer. N Engl J Med. 2004;351:1513–1520. - PubMed
-
- Scher HI, Halabi S, Tannock I, et al. Prostate Cancer Clinical Trials Working Group Design and end points of clinical trials for patients with progressive prostate cancer and castrate levels of testosterone: Recommendations of the Prostate Cancer Clinical Trials Working Group. J Clin Oncol. 2008;26:1148–1159. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
