

Bilateral posterior shoulder dislocation after electrical shock: A case report
- PMID: 26904192
- PMCID: PMC4720719
- DOI: 10.1016/j.amsu.2015.10.010
Bilateral posterior shoulder dislocation after electrical shock: A case report
Abstract
Introduction: Posterior dislocation of the shoulder is a rare and commonly missed injury. Unilateral dislocations occur mostly due to trauma. Bilateral posterior shoulder dislocations are even more rare and result mainly from epileptic seizures. Electrical injury is a rare cause of posterior shoulder dislocation. Injury mechanism in electrical injury is similar to epileptic seizures, where the shoulder is forced to internal rotation, flexion and adduction.
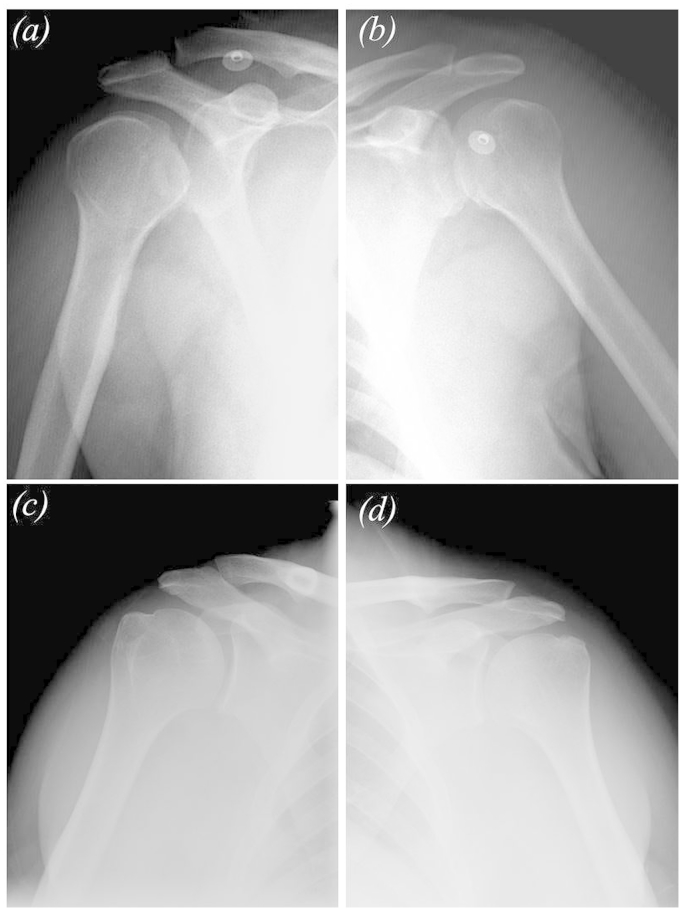
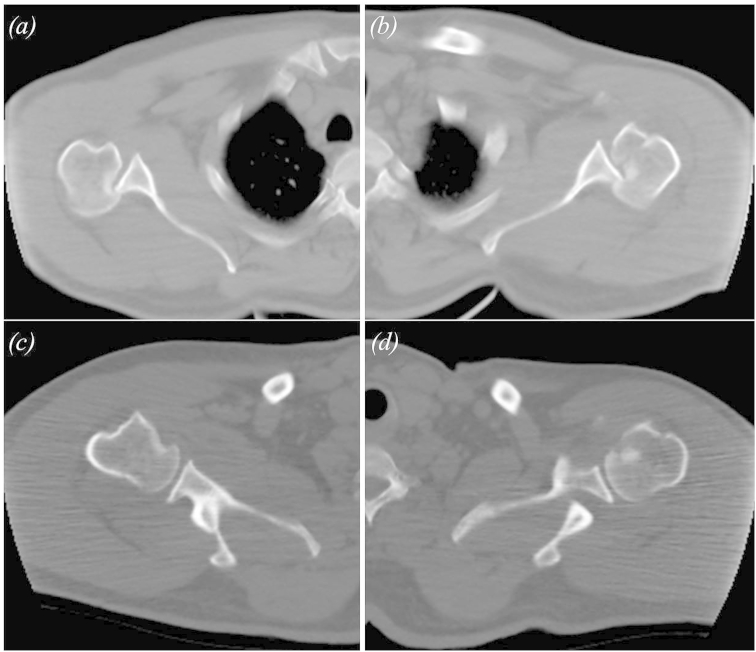
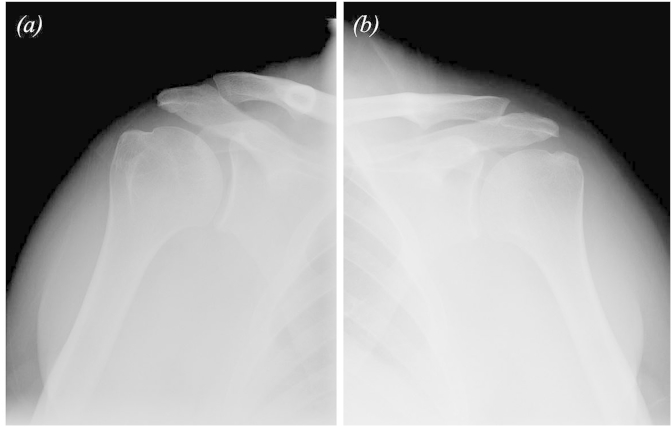
Presentation of case: This report presents a case of bilateral posterior shoulder dislocation after electrical shock. We were able to find a few individual case reports describing this condition. The case was acute and humeral head impression defects were minor. Our treatment in this case consisted of closed reduction under general anesthesia and applying of orthoses which kept the shoulders in abduction and external rotation. A rehabilitation program was begun after 3 weeks of immobilization. After 6 months of injury the patient has returned to work. 20 months postoperatively, at final follow-up, he was painless and capable of performing all of his daily activities.
Discussion: The amount of bilateral shoulder dislocations after electrical injury is not reported but is known to be very rare. The aim of this case presentation is to report an example for this rare entity, highlight the difficulties in diagnosis and review the treatment options.
Conclusion: Physical examination and radiographic evaluation are important for quick and accurate diagnosis.
Keywords: Bilateral posterior shoulder dislocation; Electrical shock; Reverse Hill-Sachs lesion.
Figures

Similar articles
-
Difficulty in Early Diagnosis of Bilateral Posterior Fracture-dislocation of the Shoulder Caused by an Electric Shock in a Walk-in Patient: A Case Report.J Orthop Case Rep. 2024 Jul;14(7):30-35. doi: 10.13107/jocr.2024.v14.i07.4564. J Orthop Case Rep. 2024. PMID: 39035384 Free PMC article.
-
Simultaneous bilateral posterior dislocation of the shoulder: diagnostic problems and management. A case report.Knee Surg Sports Traumatol Arthrosc. 2006 Aug;14(8):766-70. doi: 10.1007/s00167-006-0066-1. Epub 2006 Feb 24. Knee Surg Sports Traumatol Arthrosc. 2006. PMID: 16501951
-
Bilateral Posterior Fracture-Dislocation of the Shoulder after Electrical Shock Treated with Bilateral Hemiarthroplasty: A Case Report.Malays Orthop J. 2022 Mar;16(1):146-149. doi: 10.5704/MOJ.2203.025. Malays Orthop J. 2022. PMID: 35519525 Free PMC article.
-
Bilateral Locked Posterior Fracture-Dislocation of the Shoulder After Epileptic Seizures Secondary to Cavernous Hemangioma: A Case Report and Literature Review.Am J Case Rep. 2023 Jun 19;24:e940141. doi: 10.12659/AJCR.940141. Am J Case Rep. 2023. PMID: 37337276 Free PMC article. Review.
-
Posterior shoulder fracture-dislocation: an update with treatment algorithm.Eur J Orthop Surg Traumatol. 2017 Apr;27(3):285-294. doi: 10.1007/s00590-016-1840-5. Epub 2016 Aug 25. Eur J Orthop Surg Traumatol. 2017. PMID: 27562590 Review.
Cited by
-
Difficulty in Early Diagnosis of Bilateral Posterior Fracture-dislocation of the Shoulder Caused by an Electric Shock in a Walk-in Patient: A Case Report.J Orthop Case Rep. 2024 Jul;14(7):30-35. doi: 10.13107/jocr.2024.v14.i07.4564. J Orthop Case Rep. 2024. PMID: 39035384 Free PMC article.
-
Two Cases of Anterior Shoulder Dislocation and Fracture Secondary to Generalized Tonic-Clonic Seizure.Case Rep Orthop. 2024 Feb 7;2024:6652622. doi: 10.1155/2024/6652622. eCollection 2024. Case Rep Orthop. 2024. PMID: 38356915 Free PMC article.
-
The Power of Movement: A Comprehensive Case Study of Physiotherapeutic Approaches in Electrical Injury Rehabilitation.Cureus. 2024 Jul 15;16(7):e64615. doi: 10.7759/cureus.64615. eCollection 2024 Jul. Cureus. 2024. PMID: 39149673 Free PMC article.
-
Consecutive posterior shoulder fracture dislocation after a cerebral saccular aneurysm episode: a rare case.JSES Rev Rep Tech. 2022 May 23;2(3):391-394. doi: 10.1016/j.xrrt.2022.04.010. eCollection 2022 Aug. JSES Rev Rep Tech. 2022. PMID: 37588861 Free PMC article. No abstract available.
-
Diagnosis and treatment of posterior shoulder instability based on the ABC classification.EFORT Open Rev. 2024 May 10;9(5):403-412. doi: 10.1530/EOR-24-0025. EFORT Open Rev. 2024. PMID: 38726995 Free PMC article. Review.
References
-
- Robinson C.M., Akhtar A., Mitchell M., Beavis C. Complex posterior fracture-dislocation of the shoulder. Epidemiology, injury patterns, and results of operative treatment. J. Bone Jt. Surg. Am. 2007;89:1454–1466. - PubMed
-
- Bock P., Kluger R., Hintermann B. Anatomical reconstruction for Reverse Hill Sach lesions after posterior locked shoulder dislocation fracture: a case series of six patients. Arch. Orthop. Trauma Surg. 2007;127:543–548. - PubMed
-
- Brackstone M., Patterson S.D., Kertesz A. Triple “E” syndrome: bilateral locked posterior fracture dislocation of the shoulders. Neurology. 2001;56:1403–1404. - PubMed
-
- Shaw J.L. Bilateral posterior fracture-dislocation of the shoulder and other trauma caused by convulsive seizures. J. Bone Jt. Surg. Am. 1971;53:1437–1440. - PubMed
-
- Elberger S.T., Brody G. Bilateral posterior shoulder dislocations. Am. J. Emerg. Med. 1995;13:331–332. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
