

Granulomatous Interstitial Nephritis Presenting as Hypercalcemia and Nephrolithiasis
- PMID: 26904327
- PMCID: PMC4745585
- DOI: 10.1155/2016/4186086
Granulomatous Interstitial Nephritis Presenting as Hypercalcemia and Nephrolithiasis
Abstract
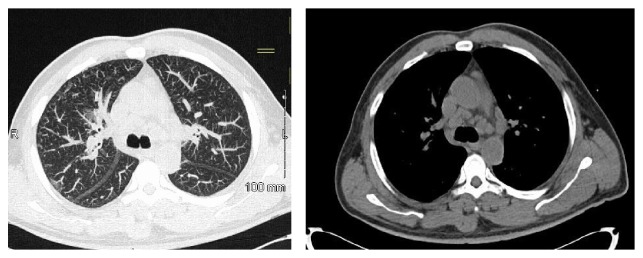
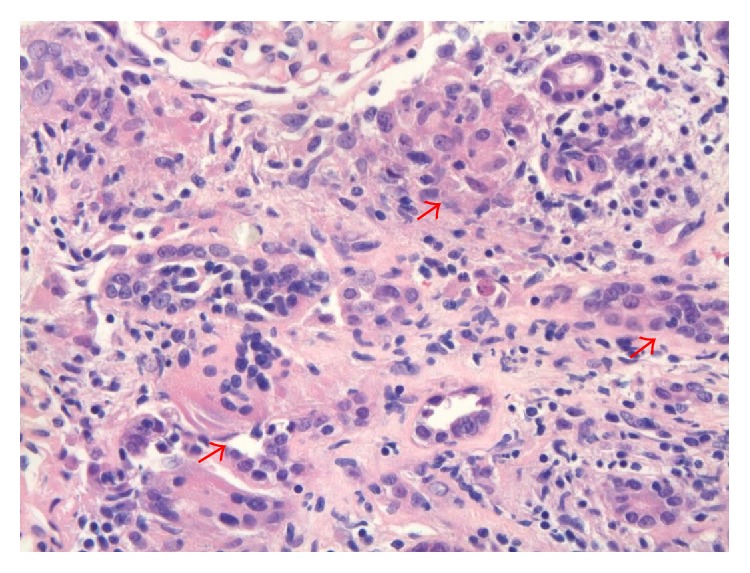
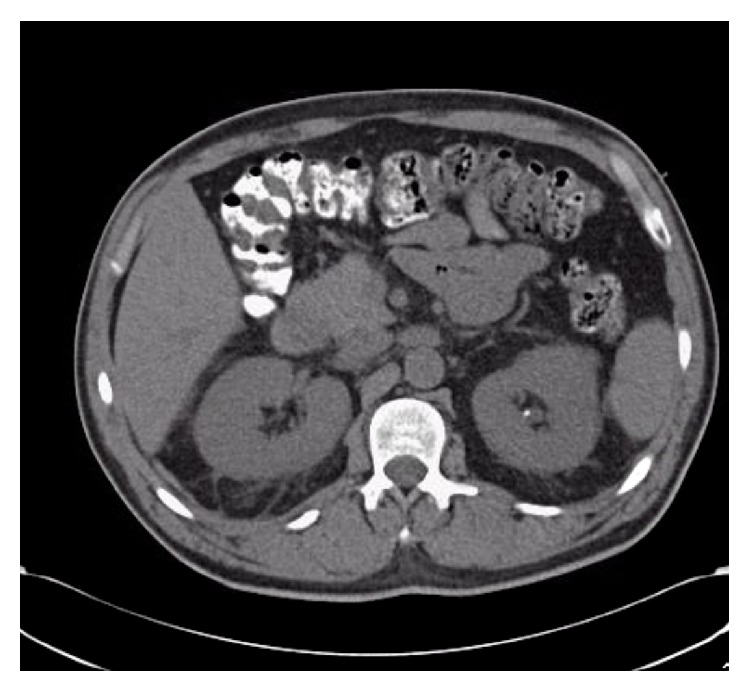
We report a case of acute kidney injury as the initial manifestation of sarcoidosis. A 55-year-old male was sent from his primary care physician's office with incidental lab findings significant for hypercalcemia and acute kidney injury with past medical history significant for nephrolithiasis. Initial treatment with intravenous hydration did not improve his condition. The renal biopsy subsequently revealed granulomatous interstitial nephritis (GIN). Treatment with the appropriate dose of glucocorticoids improved both the hypercalcemia and renal function. Our case demonstrates that renal limited GIN due to sarcoidosis, although a rare entity, can cause severe acute kidney injury and progressive renal failure unless promptly diagnosed and treated.
Figures
Similar articles
-
Renal sarcoidosis presenting as acute kidney injury with granulomatous interstitial nephritis and vasculitis.Am J Kidney Dis. 2012 Feb;59(2):303-8. doi: 10.1053/j.ajkd.2011.09.025. Epub 2011 Dec 15. Am J Kidney Dis. 2012. PMID: 22177616
-
Sarcoidosis and the kidney: not only the granulomatous interstitial nephritis.Clin Nephrol. 2009 Feb;71(2):192-5. doi: 10.5414/cnp71192. Clin Nephrol. 2009. PMID: 19203514
-
A case of acute kidney injury caused by granulomatous interstitial nephritis associated with sarcoidosis.CEN Case Rep. 2018 May;7(1):34-38. doi: 10.1007/s13730-017-0287-9. Epub 2017 Nov 27. CEN Case Rep. 2018. PMID: 29181823 Free PMC article.
-
[Rapidly progressing renal insufficiency as the primary manifestation of systemic sarcoidosis].Med Klin (Munich). 1999 Dec 15;94(12):690-4. doi: 10.1007/BF03044760. Med Klin (Munich). 1999. PMID: 10641512 Review. German.
-
Granulomatous interstitial nephritis.Clin Kidney J. 2015 Oct;8(5):516-23. doi: 10.1093/ckj/sfv053. Epub 2015 Jul 5. Clin Kidney J. 2015. PMID: 26413275 Free PMC article. Review.
Cited by
-
AKI and Hypercalcemia in a Patient with Weakness and Fatigue.Kidney360. 2020 Nov 25;1(11):1328-1329. doi: 10.34067/KID.0002282020. eCollection 2020 Nov 25. Kidney360. 2020. PMID: 35372880 Free PMC article. No abstract available.
-
Malignant Hypercalcemia Revealing Pulmonary Sarcoidosis.Cureus. 2024 Jul 13;16(7):e64454. doi: 10.7759/cureus.64454. eCollection 2024 Jul. Cureus. 2024. PMID: 39135824 Free PMC article.
-
Idiopathic granulomatous interstitial nephritis and isolated renal sarcoidosis: Two diagnoses of exclusion.SAGE Open Med. 2021 Aug 13;9:20503121211038470. doi: 10.1177/20503121211038470. eCollection 2021. SAGE Open Med. 2021. PMID: 34408878 Free PMC article. Review.
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
