

Inverted Internal Limiting Membrane Flap Technique for Repair of Large Macular Holes: A Short-term Follow-up of Anatomical and Functional Outcomes
- PMID: 26904983
- PMCID: PMC4804430
- DOI: 10.4103/0366-6999.176988
Inverted Internal Limiting Membrane Flap Technique for Repair of Large Macular Holes: A Short-term Follow-up of Anatomical and Functional Outcomes
Abstract
Background: Inverted internal limiting membrane (ILM) flap technique has recently been reported in a limited number of studies as an effective surgical technique for the management of large macular holes (MHs) with fair MH closure rates as well as gains in visual acuity. In the current study, longitudinal changes in multi-focal electroretinogram (mfERG) responses, best-corrected visual acuity (BCVA) and spectral-domain optical coherence tomography (SD-OCT) were evaluated in eyes with large MHs managed by this technique.
Methods: A prospective noncontrolled interventional study of eight patients (eight eyes) with large MHs (minimum diameter >400 μm) was conducted. All MHs were treated with pars plana vitrectomy and indocyanine green-assisted inverted ILM flap technique. SD-OCT images were used to assess the anatomical outcomes of surgery while BCVA and mfERG were used to evaluate the functional outcomes during a 3-month follow-up.
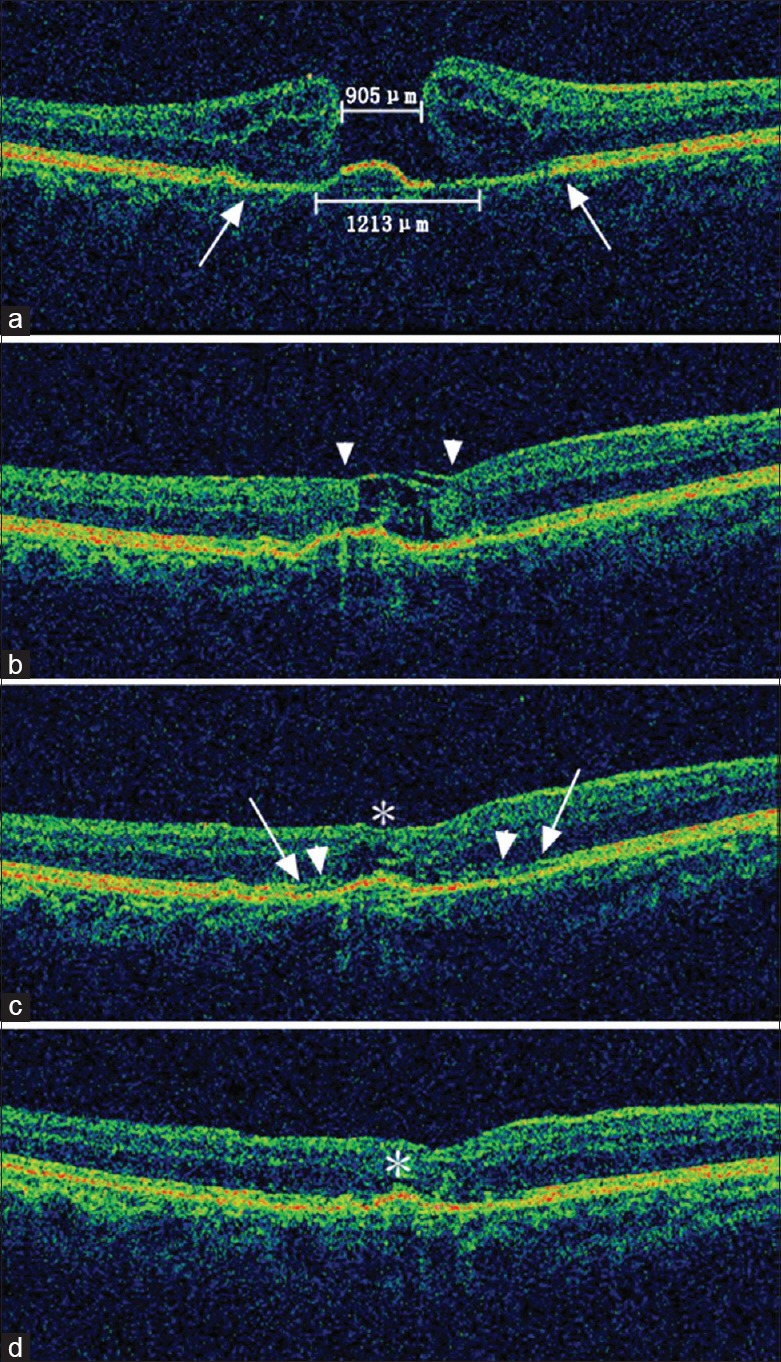
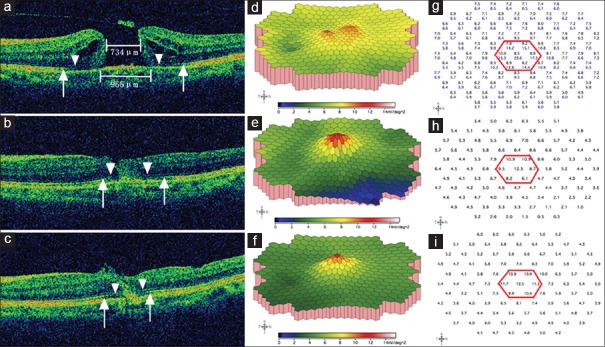
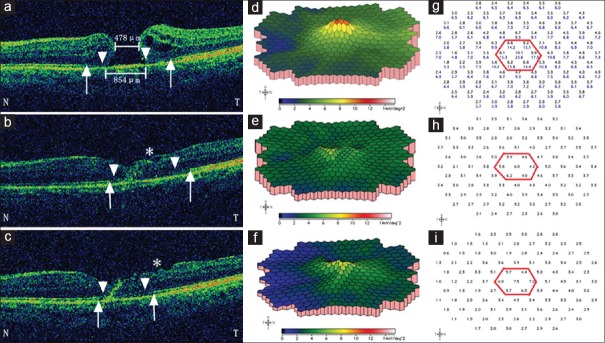
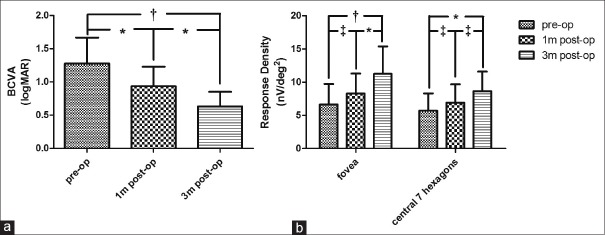
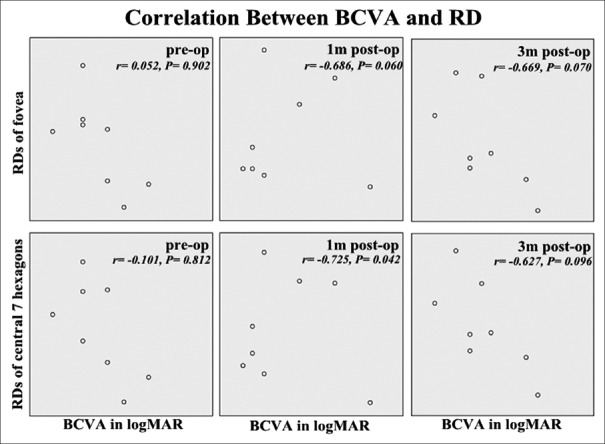
Results: All patients underwent successful intended manipulation and translocation of the ILM flap without flap dislocation and achieved complete anatomical closure. Partial microstructural reconstruction, demonstrated on SD-OCT as restoration of the external limiting membrane and the ellipsoid zone, was observed in all cases as early as 1 month after surgery. Functionally, as compared to baseline, all patients showed improvements in BCVA and all but one in mfERG response during follow-up. However, Pearson's test revealed no significant correlations between BCVA and mfERG responses of the fovea and of the macular area at each evaluation time point.
Conclusions: Inverted ILM flap technique appears to be a safe and effective approach for the management of large idiopathic MHs with favorable short-term anatomical and functional results. Postoperative reconstruction of the microstructure generally shows good consistency with improvements in both BCVA and mfERG response, of which the latter might be a supplement for the former in postoperative functional follow-up.
Figures
References
-
- Welly NE, Wendel RT. Vitreous surgery for idiopathic macular holes. Results of a pilot study. Arch Ophthalmol. 1991;109:654–9. - PubMed
-
- Kadonosono K, Itoh N, Uchio E, Nakamura S, Ohno S. Staining of internal limiting membrane in macular hole surgery. Arch Ophthalmol. 2000;118:1116–8. - PubMed
-
- Ando F, Sasano K, Ohba N, Hirose H, Yasui O. Anatomic and visual outcomes after indocyanine green-assisted peeling of the retinal internal limiting membrane in idiopathic macular hole surgery. Am J Ophthalmol. 2004;137:609–14. - PubMed
-
- Beutel J, Dahmen G, Ziegler A, Hoerauf H. Internal limiting membrane peeling with indocyanine green or trypan blue in macular hole surgery: A randomized trial. Arch Ophthalmol. 2007;125:326–32. - PubMed
-
- Henrich PB, Haritoglou C, Meyer P, Ferreira PR, Schötzau A, Katamay R, et al. Anatomical and functional outcome in brilliant blue G assisted chromovitrectomy. Acta Ophthalmol. 2010;88:588–93. doi: 10.1111/j.1755-3768.2008.01477.x. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
